
Remember me



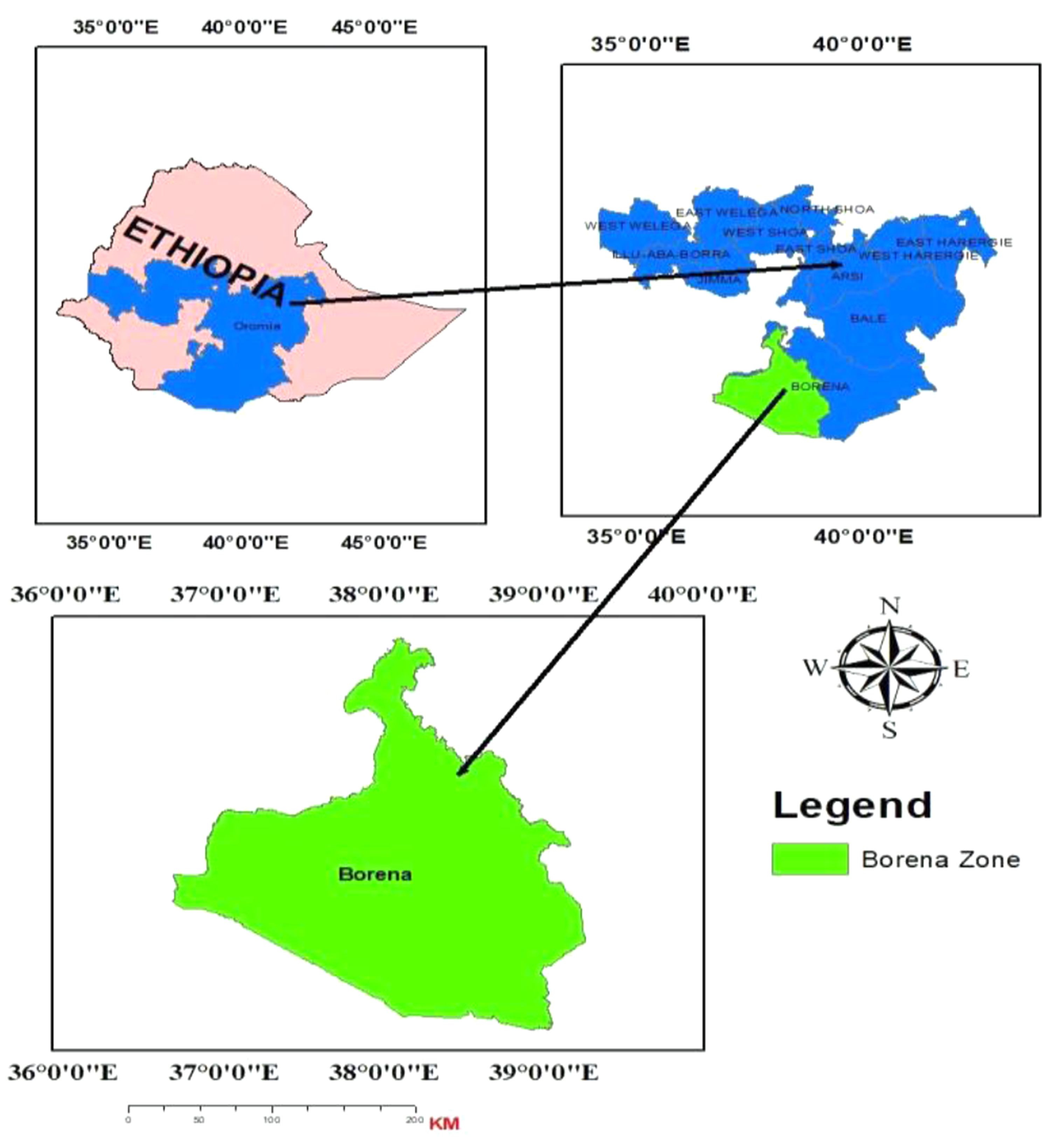

The study was conducted at Yabelo General Hospital, situated in Yabelo town, Borena Zone. This zone is one of twenty-one zones in the Oromia Region. In 2010, the hospital was upgraded from a Health Center to a general hospital. It provides various services to the residents of Borena Zone and other Ethiopian ethnic groups. Currently, the zone comprises ten rural pastoralist woredas and one town administration, Yabelo, which has a state function. The zone is located in the southern part of the Oromia region. It shares borders with the West Guji Zone to the north, the South Nations, Nationalities, and Peoples region to the west, the Somali region to the southeast, and an international boundary with Kenya to the south (as shown in the geographical map below, Fig. 1).
Fig. 1
According to the 2023 report from the Borena Zone Administration Office, over 1.4 million people reside in the zone, with a male-to-female ratio of 1:1. This suggests significant variation in settlement patterns from district to district. Approximately 89% of the population inhabits the rural pastoralist areas of the zone [10]. The Borana Zone is one of the most pastoralist regions in Ethiopia, primarily relying on livestock rearing. The livestock population in Borena includes 1,482,053 goats, 1,179,645 sheep, 637,632 horses, 2,222 mules, 5,525 donkeys, 68,799 camels, and 185,382 cattle [11].
Source of data and study populationThe study is a retrospective cohort analysis, indicating that all events and exposures detailed in the review subjects’ patient cards and information sheets occurred in the past. All individuals diagnosed with HIV at Yabelo General Hospital and receiving ART were included in the study at regular intervals. Based on the inclusion and exclusion criteria, 293 adult HIV/AIDS patients were selected from their medical records. Participants in this study were HIV-positive individuals receiving follow-up antiretroviral therapy during the study intervals. This study encompassed all adult HIV-positive patients who visited the hospital for treatment three or more times, as well as adult HIV/AIDS patients who initiated treatment between January 2016 and December 2019. According to hospital records, 1,147 HIV patients underwent ART treatment and were assessed for baseline CD4 count cells during the study periods.
Sample size determinationThe researcher was able to obtain statistically significant results by employing the formula for calculating the required sample size [12]. According to [13], the sample size was determined by analyzing the mortality rates in two groups of HIV-positive individuals on ART, categorized by their WHO clinical stage as exposure status. Consequently, the sample size for this current study has reached 293 HIV/AIDS-positive subjects, taking into account the inclusion criteria (further calculations are available in the supplementary material).
Variables of the studyThe outcome variable for survival analysis is the survival time and/or time to death of patients under follow-up among HIV-infected adults. The predictors included in this study were gender, age, marital status, educational status, place of residence, WHO stages, TB, adherence to ART treatment, functional status, family history, and opportunistic infectious diseases.
WHO stagesThese are the clinical stages of patients based on CD4 values, classified into four stages: stage I, stage II, stage III, and stage IV.
Tuberculosis (TB)Individuals with HIV and weakened immune systems are at a higher risk of contracting tuberculosis compared to those with typical immune systems.
Family HistoryThis refers to the previous occurrences of HIV/AIDS disease or past incidences among family members.
Opportunistic infectious diseasesThese are infections that occur more frequently and are more severe in individuals with declining immune systems.
Functional statusWorking: able to perform usual work in or out of the house; Ambulatory: able to carry out activities of daily living; Bedridden: unable to perform activities of daily living [14].
AdherenceAdherence was categorized as good if patients adhered to at least 95% of the prescribed medication, fair if they adhered between 85% and 95%, and poor if they adhered to less than 85% of the prescribed medication [15].
Method of analysisThe analysis was conducted using R software version 4.3.1. It includes descriptive statistics of variables, the Kaplan-Meier method, the log-rank test, and the Cox proportional hazards model for the time-to-event data from the survival datasets.
Survival analysis modelSurvival analysis is a branch of statistics that investigates the anticipated duration until one or more events take place [16]. This data shows that not all patients experience the event by the conclusion of the observation period; thus, the actual survival times for some individuals living with HIV/AIDS remain unknown, a phenomenon referred to as censoring, which must be accounted for in the study to yield meaningful results [17, 18].
Kaplan - Meier estimatorThe Kaplan-Meier estimator [19] provides a non-parametric maximum likelihood estimate of the survival function.
Cox proportional hazards modelThe basic model for survival analysis is investigated under the Cox proportional hazard model, a model originated by Cox [16]. In a model, the unique effect of a unit increase in a covariate is multiplicative in terms of the hazard rate. Its covariates can be time-independent. This model implies that the hazard function \(\:_\)(t, X,)\(\:\beta\:\) is connected to the covariates as a product of a baseline hazard \(\:}_\left(\text\right)\) and a function of covariates.
Comments (0)