
Remember me




Our study demonstrated a significant positive association between elevated AIP and incident diabetes in both Chinese and Japanese populations. This association remained robust after comprehensive adjustment for potential confounders, including demographic characteristics, lifestyle factors, and metabolic parameters. The relationship exhibited a dose-dependent pattern, with higher AIP quartiles consistently associated with greater diabetes risk. Furthermore, we observed non-linear relationships between AIP and diabetes risk, with identifiable threshold effects differing between Chinese and Japanese populations. Subgroup analyses revealed that the association was modified by age, BMI, and systolic blood pressure, while mediation analysis indicated that BMI partially mediated the effect of AIP on diabetes development.
In this study, we found that the overall diabetes incidence rate in the Chinese population was 1.27% (95% CI: 1.20–1.34%), while the Japanese population showed a significantly higher incidence of 2.41% (95% CI: 2.17–2.66%). This difference was consistent across all age groups, particularly pronounced in middle-aged and elderly populations between 40 and 70 years, with Japanese males over 70 years showing the highest diabetes incidence rate of nearly 7.14%. This difference in incidence rates may reflect variations in dietary patterns, lifestyle, and genetic factors between the two countries[43]. While rich in fish and vegetables, the traditional Japanese diet also contains a high proportion of refined carbohydrates such as white rice, which may lead to increased postprandial glucose fluctuations [44]. Additionally, Japanese populations generally face higher work stress and less physical activity, which have been established as independent risk factors for diabetes [45]. From a genetic perspective, studies have suggested that specific genetic variants in the Japanese population, such as polymorphisms in TCF7L2 and KCNQ1 gene loci, may increase susceptibility to diabetes[46]. Moreover, follow-up duration may also influence the difference in diabetes incidence rates between Chinese and Japanese populations. In this study, the maximum follow-up period for the Chinese cohort was approximately 7 years, while for the Japanese cohort it was around 12 years. Therefore, the incidence rate in the Japanese population might be relatively higher.
Moreover, we observed that the dose-effect relationship between AIP quartiles and diabetes incidence was steeper in the Japanese population, rising sharply from 0.84% in Q1 to 7.30% in Q4, compared to the Chinese population, which increased from 0.40% in Q1 to 2.49% in Q4. This suggests that elevated AIP levels may have a stronger impact on diabetes risk in the Japanese population, possibly related to their unique metabolic characteristics and lipid metabolism patterns[47].
After comprehensive adjustment for potential confounding factors, our study found a significant positive association between AIP and diabetes risk, consistent with previous research [15, 17]. In the fully adjusted model, each unit increase in AIP was associated with a 1.39-fold increase in diabetes risk in the overall population (HR: 2.390, 95% CI: 2.047–2.792), a 84% increase in the Chinese population (HR: 1.843, 95% CI: 1.540–2.206), and a 1.42-fold increase in the Japanese population (HR: 2.420, 95% CI: 1.665–3.516). These findings align with those of Yin et al. in the U.S. population, who reported that AIP was positively associated with insulin resistance and type 2 diabetes risk [13]. Notably, although the HR value for the Japanese population (2.42) appeared higher than that for the Chinese population (1.84) in the Cox regression analysis, our subgroup analysis showed that the interaction test by country did not reach statistical significance (P for interaction = 0.1974). This suggests that the strength of the association between AIP and diabetes may not substantially differ between the two populations, and the apparent difference might be attributed to imbalanced sample sizes and random variation. This finding enhances the robustness of our results, indicating that despite racial and cultural differences, the value of AIP as a marker of diabetes risk is consistent across different East Asian populations.
Sensitivity analyses further supported the robustness of the association between AIP and diabetes risk. In models excluding obese individuals, smokers, drinkers, and those with hypertriglyceridemia, the significant positive association between AIP and diabetes risk persisted. Particularly in individuals with normal triglyceride levels (< 1.7mmol/L), AIP remained significantly associated with diabetes risk (HR: 2.236, 95% CI: 1.623–3.080), suggesting that AIP may influence diabetes risk through mechanisms beyond merely reflecting elevated triglyceride levels [48].
Subgroup analyses revealed several essential effect modifiers. Age significantly influenced the association between AIP and diabetes risk (P for interaction = 0.0003), with the strongest associations observed in young (20–45 years) and middle-aged (45–60 years) populations, and weaker associations in the elderly (≥ 60 years). This is consistent with Sun et al.‘s findings that the association between AIP and type 2 diabetes weakened with increasing age (interaction P < 0.001) [16]. This age-dependent effect may reflect age-related changes in lipid metabolism and declining pancreatic function [49].
Using restricted cubic spline curves and piecewise Cox regression models, our study revealed a significant non-linear relationship between AIP and diabetes risk, with different inflection points identified in different populations. In the overall population, the inflection point was AIP = 0.432, below which each unit increase in AIP was associated with a nearly 2-fold increase in diabetes risk (HR = 2.956), while above this threshold, the association was no longer significant. The Chinese population exhibited a similar pattern to the overall population, with an inflection point at AIP = 0.436, below which the association was strong (HR = 2.180) and above which it was non-significant. This finding partially supports the study by Zhu et al. in non-obese Chinese adults, who identified a clinically significant threshold of -0.02 [15], but also differs from ours. This discrepancy may stem from differences in study population characteristics (such as including obese individuals in our study) and follow-up duration.
Interestingly, the Japanese population demonstrated an opposite pattern, with an inflection point at AIP=-0.449, below which the association was non-significant, while above this threshold it was strongly significant (HR = 2.842). This is similar to the J-shaped relationship observed by Zhou et al. in the Japanese population, who reported significantly increased type 2 diabetes risk when AIP exceeded − 0.268 [17].
The differences in non-linear relationship patterns between Chinese and Japanese populations may reflect multiple differences in genetic background and environmental exposure. First, the genetic basis of lipid metabolism may vary across different East Asian populations, with studies suggesting that specific gene polymorphisms can influence lipoprotein levels and insulin sensitivity[50]. Second, dietary pattern differences (such as higher seafood intake and specific fatty acid composition in the Japanese population) may influence lipid metabolism pathways and insulin resistance development[51]. Third, environmental factors such as physical activity patterns, occupational stress, and degrees of urbanization may collectively shape the population-specific manifestations of this non-linear relationship [52].
Our findings regarding the differential impact of AIP thresholds across different populations align with recent high-quality systematic reviews on cardiometabolic interventions. For example, in a meta-analysis on the effects of flaxseed supplementation in diabetic patients [11], researchers found that flaxseed effectively reduced anthropometric indices and triglyceride levels, particularly in long-term (> 12 weeks) interventions. However, similar to our findings on population-specific responses, they observed that baseline characteristics (including age and BMI) significantly moderated the intervention effects, supporting our argument for the necessity of individualized risk assessment.
Furthermore, the systematic review on the effects of purslane on glycemic indices[53] also supports the concept of population-specific responses to metabolic indicators. Their analysis showed that purslane supplementation significantly reduced fasting blood glucose across all populations, but its effects on insulin resistance markers differed significantly based on health status and demographic factors. This pattern of differential responses across different populations mirrors the variation in AIP thresholds we observed between different populations, highlighting the importance of considering population-specific differences when evaluating cardiometabolic risk factors.
Additionally, in their network meta-analysis on pharmacological interventions for youth obesity[54], researchers demonstrated that different medications had varying impacts on cardiometabolic risk factors, with some effectively improving anthropometric measures but not correspondingly improving lipid profiles and blood pressure. For instance, they found that high-dose phentermine/topiramate effectively reduced anthropometric measures, while orlistat better improved diastolic blood pressure, emphasizing the complex relationships between different cardiometabolic risk factors. This approach of comprehensively assessing multiple cardiometabolic risk factors aligns with our research methodology, where we focus on AIP as an indicator that integrates multiple lipid parameters and explores its relationship with diabetes risk.
Notably, the systematic review, meta-analysis, and GRADE assessment on the effect of berberis (Vulgaris and Integerrima) on cardiovascular risk factors in patients with type 2 diabetes mellitus [55]found that berberis supplementation effectively improved lipid profiles (triglycerides, total cholesterol, and low-density lipoprotein cholesterol) and glycemic indices. This study particularly emphasized the importance of evidence-based medicine approaches in evaluating the efficacy of metabolic interventions and provided strong evidence for berberis in improving AIP-related lipid parameters. These findings further support our conclusion that the impact of interventions on cardiometabolic risk factors is moderated by multiple factors that should be incorporated into personalized prevention and treatment strategies.
These comparative findings from recent high-quality systematic reviews and meta-analyses [11, 53–55] reinforce our conclusion that metabolic pathways and intervention responses differ across ethnic groups, necessitating population-specific approaches to cardiometabolic risk assessment and management. The differential threshold effects of AIP on diabetes risk that we observed between different populations may reflect fundamental differences in lipid metabolism, fat distribution, and insulin sensitivity pathways—differences that should inform personalized prevention strategies.
Our study revealed distinct AIP threshold values associated with increased T2DM risk in Chinese and Japanese populations. These differences should be interpreted within the context of substantial baseline characteristic variations between the cohorts. The Japanese cohort demonstrated significantly higher rates of smoking (41.6% vs. 20.4%) and alcohol consumption (69.4% vs. 16.5%), along with different metabolic profiles, including lipid parameters that directly influence AIP calculation. These differences reflect the distinct lifestyle patterns, dietary habits, and potentially environmental exposures characteristic of these populations.
Rather than undermining our findings, these population differences highlight the importance of establishing population-specific clinical thresholds that account for the unique constellation of risk factors and metabolic characteristics present in different groups. Despite these differences, the consistent association between AIP and T2DM risk across both populations strengthens the case for AIP as a robust indicator while simultaneously demonstrating the necessity of calibrating risk thresholds to specific population contexts.
The observed threshold differences likely result from complex interactions between multiple factors. Dietary patterns differ substantially between Chinese and Japanese populations, with variations in carbohydrate intake, types of dietary fats, and consumption of specific food groups like seafood and fermented products that may influence lipid metabolism. Physical activity patterns, body composition differences beyond BMI, and potentially genetic factors affecting lipid metabolism may further contribute to the observed threshold variations. Additionally, differences in healthcare systems and screening practices between countries may influence the timing of T2DM diagnosis.
This study evaluated AIP’s ability to predict diabetes risk, showing that AIP has good predictive value in both populations. However, we found important differences when comparing ROC curves between Chinese and Japanese populations. In the Japanese population, AIP’s ability to predict diabetes appeared superior to that in the Chinese population, which may reflect differences in the association between lipid metabolism abnormalities and diabetes development between the two populations. In the Japanese population, lipid metabolism abnormalities may be stronger predictors of diabetes development, consistent with the steeper dose-response relationship between AIP and diabetes risk observed in this population. Potential explanations for this difference in predictive performance include: First, the Japanese population may have unique lipid metabolism characteristics that make AIP a more sensitive predictor of diabetes risk [56]. Previous studies have suggested that despite lower BMI, Japanese individuals may face a higher risk of visceral fat accumulation, which is closely related to insulin resistance [57]. Second, dietary factors such as seafood consumption may influence lipid metabolism and insulin sensitivity [44]. Third, genetic factors may regulate lipid metabolism and glucose tolerance differently in the two populations [58].
Compared with previous studies, our AIP prediction model’s performance is generally consistent with Sun et al.‘s findings in the Chinese obese population[16], but slightly higher than the results reported by Zhou et al. in the Japanese population[17]. These differences may reflect methodological variations, including follow-up time, adjustment factors, and diagnostic criteria. Overall, our ROC analysis results not only support AIP as a valuable tool for predicting diabetes risk in East Asian populations but also emphasize the importance of population-specific reference values, which have important implications for clinical practice.
Mediation analysis revealed that BMI plays an important partial mediating role in the relationship between AIP and diabetes development. In the overall population, BMI mediated 37.27% of the total effect, suggesting that AIP influences diabetes risk through two pathways: an indirect pathway through BMI (AIP→BMI→diabetes) and a direct pathway independent of BMI (AIP→diabetes). Interestingly, we found that the mediation effect differed between the two populations. In the Chinese population, BMI mediated 39.84% of the total effect, while in the Japanese population, this proportion was only 27.11%. This suggests that in the Chinese population, AIP’s impact on diabetes risk is more mediated through obesity, while in the Japanese population, the direct effect is more pronounced.
Several factors may contribute to these observed variations regarding the differences in mediation proportions between Chinese (39.84%) and Japanese (27.11%) populations. These include biological, lifestyle, and methodological considerations that warrant careful interpretation.
From a biological perspective, research has documented ethnic variations in lipid metabolism and obesity-related diabetes risk among Asian populations. Yaghootkar et al.‘s research revealed that different ethnicities have genetic predispositions for differences in adipose tissue expansion capacity and fat storage efficiency [59]. Wulan et al.‘s review indicated that Asians have a higher body fat percentage, more pronounced abdominal obesity, and higher intramuscular lipid content than other ethnicities at the same BMI[60], which may influence the metabolic risk profile. Within Asian populations, Seah et al. compared type 2 diabetes risk differences among East Asian, South Asian, and Southeast Asian populations, finding that body fat distribution plays an important role in diabetes risk associations across different ethnicities [61]. They noted that adjusting for BMI explained many of the observed ethnic differences, suggesting that body composition measurements and their relationship to metabolic outcomes may vary among Asian populations. Lifestyle and dietary factors may also contribute to these differences. Le et al. compared cardiometabolic risk profiles between Chinese and Finnish adults with central obesity, finding significant differences in risk factors even when controlling for demographic variables [62]. They particularly emphasized that Chinese elderly individuals exhibit lipid metabolism dysfunction that differs from Finnish populations, indicating that dietary patterns and lifestyle factors play important roles in lipid metabolism across different populations.
From a methodological perspective, our observed differences may also reflect measurement variability, unmeasured confounding, or inherent baseline differences between cohorts. Mente et al.‘s study showed that Chinese populations have the lowest BMI and abdominal adiposity[63], and these baseline differences may affect the interpretation of mediation analysis results. While our findings suggest potentially population-specific biological pathways in the AIP-BMI-diabetes relationship, we cannot rule out that these differences may be influenced by methodological factors rather than genuine biological variation. This underscores the need for prospective studies to compare these relationships across well-characterized Asian populations.
From a physiological mechanism perspective, the indirect pathway through which AIP affects diabetes risk via BMI may involve the following processes: First, lipid metabolism disorders reflected by high AIP may promote adipose tissue expansion and ectopic fat deposition [4]; second, increased free fatty acids and inflammatory factors released from adipose tissue may impair insulin sensitivity [64]; finally, persistent insulin resistance ultimately leads to pancreatic β-cell dysfunction and diabetes onset[65]. The direct effect of AIP may reflect other mechanisms, such as increased small dense low-density lipoprotein particles leading to oxidative stress and vascular endothelial dysfunction [66], as well as lipid peroxidation and pancreatic β-cell apoptosis [67]. High levels of AIP are often associated with a state of chronic inflammation in the body. Chronic inflammation can impair pancreatic β-cell function, diminishing insulin secretion capacity and increasing diabetes risk[68]. Notably, inflammatory mediators such as tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6) play a vital role in this process[69]. These findings highlight the potential value of AIP in diabetes risk assessment and suggest that regulating lipid metabolism may be an important strategy for diabetes prevention.
Based on our supplementary analyses in the Japanese cohort, we found a stronger correlation between AIP and FLI (r = 0.685) compared to AIP and WHR (r = 0.444), suggesting that AIP may be more closely linked to hepatic steatosis than visceral adiposity. This aligns with recent literature indicating that AIP reflects insulin resistance associated with fatty liver[41]. Our Cox proportional hazards models revealed that when adjusting for FLI (Adjust II-b model), the association between AIP and diabetes risk was attenuated from HR 3.520 (95% CI: 2.432–5.093) to 2.344 (95% CI: 1.481–3.709), representing a 33.4% reduction in effect size. In contrast, adjustment for WHR (Adjust II-a model) resulted in only a 6.6% reduction (HR: 3.286, 95% CI: 2.269–4.759). The mediation analysis further quantified these relationships, demonstrating that FLI mediated 23.78% of the AIP-diabetes association, while WHR mediated only 7.30%. This substantiates the hypothesis that hepatic steatosis plays a more prominent role than visceral adiposity in the pathway linking AIP to diabetes risk in Japanese adults. Interestingly, our subgroup analyses showed that the AIP-diabetes relationship remained consistent across all FLI categories (P for interaction = 0.692), suggesting that AIP predicts diabetes risk independently of baseline hepatic steatosis status. However, we observed a trend toward stronger associations in individuals with lower WHR quartiles (HR in Q1: 6.368 vs. HR in Q4: 2.830), though this interaction did not reach statistical significance (P = 0.176). These findings collectively suggest that the atherogenic lipid profile captured by AIP may contribute to diabetes risk partially through mechanisms related to hepatic fat accumulation, which aligns with the lipotoxicity theory of type 2 diabetes pathogenesis. The residual direct effect of AIP on diabetes risk after accounting for both FLI and WHR indicates that additional pathophysiological pathways likely exist beyond hepatic steatosis and visceral adiposity.
The results of this study have important clinical and public health implications. First, we confirm that AIP is a strong predictor of diabetes risk in East Asian populations, even after adjusting for traditional risk factors. As a simple, economical, and widely available biomarker, AIP can help clinicians more accurately identify high-risk individuals, especially in resource-limited healthcare settings[70]. Second, our findings of non-linear relationships and population-specific thresholds have important screening value. For the Chinese population, an AIP value of 0.436 may represent an important alert threshold, while the corresponding threshold for the Japanese population is -0.449. The differences in these thresholds emphasize the necessity of developing population-specific guidelines rather than adopting uniform global standards. Third, subgroup analysis results suggest that prevention strategies targeting specific high-risk populations (such as young to middle-aged adults, normal weight to mildly overweight individuals, and those with normal blood pressure) may be particularly effective. In these populations, the association between AIP and diabetes risk is strongest, suggesting that early regulation of lipid metabolism may yield the greatest preventive benefits[71]. Fourth, the BMI mediation analysis results indicate the importance of multi-target intervention strategies. In the Chinese population, weight management may be more critical, while in the Japanese population, interventions directly targeting lipid metabolism disorders (such as improving diet quality, increasing physical exercise, or appropriate pharmacological therapy) may be more important[72]. Finally, this study suggests that AIP may be a useful indicator for evaluating the effectiveness of diabetes prevention and lipid regulation interventions. Targeted reduction of AIP may be an important goal for future intervention studies, especially for high-risk individuals identified based on population-specific thresholds.
Our findings suggest that the AIP, as a key indicator of type 2 diabetes risk, can provide targeted prevention strategies for East Asian populations. Based on changes in AIP, the following targeted health interventions can be implemented:
(1) Personalized Dietary Interventions: Tailored dietary advice based on AIP and BMI levels for high-risk individuals could involve increasing the intake of foods rich in monounsaturated fatty acids (such as nuts and fish) to improve lipid metabolism and subsequently reduce diabetes risk.
(2) Lifestyle Modifications: Encouraging high-risk individuals to increase physical activity and improve lifestyle can significantly lower AIP levels and reduce the risk of developing diabetes. Regular health checks and health education should also be included in preventive strategies.
(3) Early Screening and Monitoring: Regular screening protocols for individuals with elevated AIP can be crucial in implementing early interventions to decrease the likelihood of diabetes onset, especially in high-risk populations.
This study has several important strengths. First, we employed a large prospective cohort design, covering two East Asian populations with different lifestyles and environmental exposures but similar genetic backgrounds, enhancing our findings’ external validity. Second, we implemented comprehensive data adjustment and analytical strategies, including multivariate Cox regression, sensitivity analyses, subgroup analyses, non-linear relationship exploration, and mediation analysis, providing a comprehensive perspective on the relationship between AIP and diabetes. Third, we used piecewise regression models to identify population-specific thresholds for the relationship between AIP and diabetes risk, providing concrete reference points for clinical practice. Fourth, our study is the first systematic comparison of the association patterns between AIP and T2DM risk across different East Asian populations, filling an important knowledge gap in this field. Fifth, we employed innovative statistical methods to assess the mediating role of BMI in the AIP-diabetes relationship, revealing potential pathogenic mechanisms that offer new insights for targeted interventions. Finally, our findings have clear clinical translation value, with the proposed population-specific AIP thresholds serving as reference standards for risk assessment and early intervention.
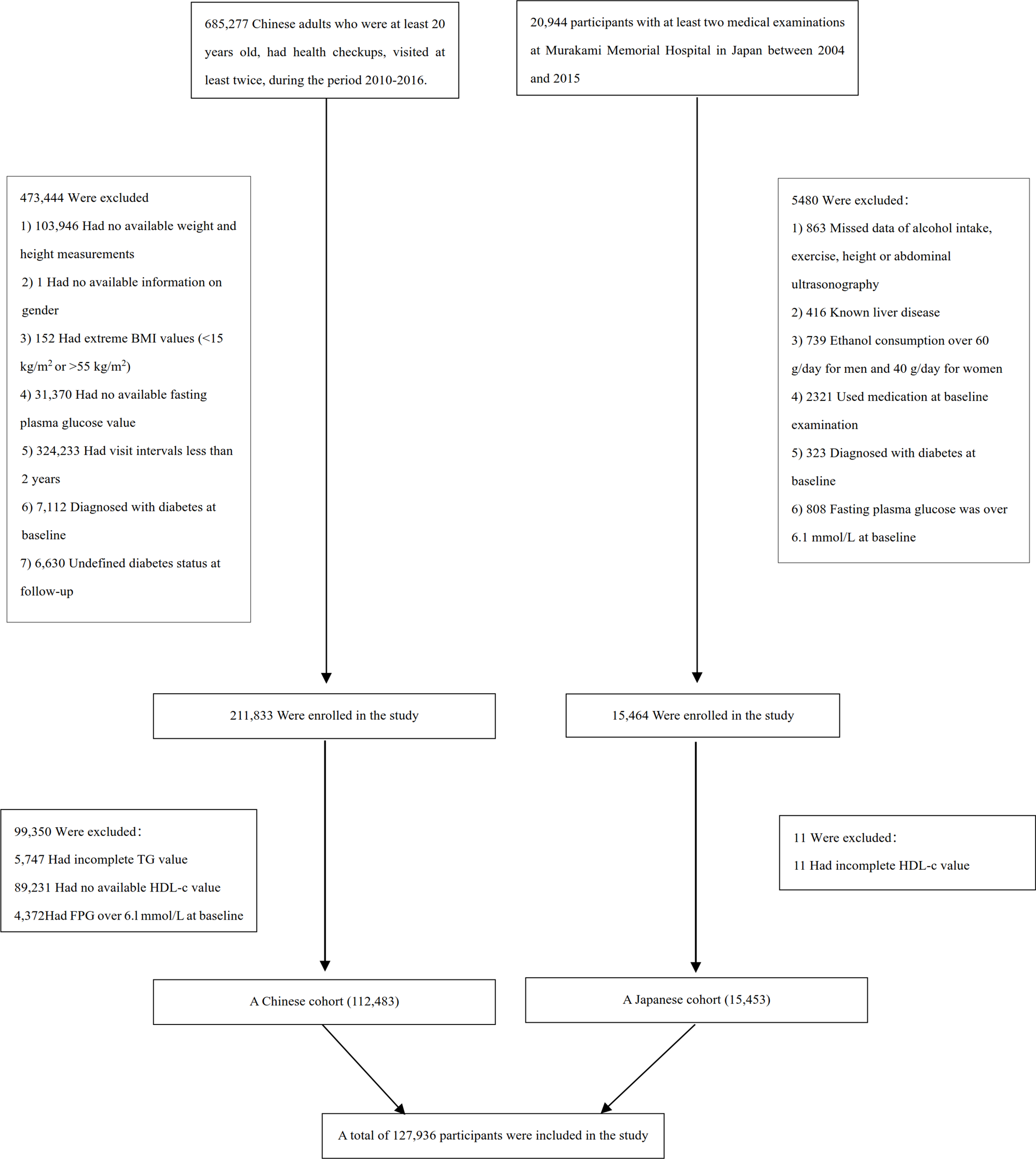
However, this study also has several limitations. First, there is a substantial difference in follow-up time and sample size between the Chinese (n = 112,483) and Japanese (n = 15,453) cohorts, necessitating separate analyses rather than direct statistical comparisons. While both cohorts maintained adequate statistical power for primary analyses, the smaller Japanese cohort may have limited power for detecting subtle effects in some subgroup analyses. Second, the baseline characteristics between cohorts demonstrated profound differences extending beyond expected demographic variations, including smoking rates (Chinese 20.4% vs. Japanese 41.6%), alcohol consumption patterns (Chinese 16.5% vs. Japanese 69.4%), and multiple metabolic parameters. These systematic differences indicate that these cohorts represent different populations with distinct lifestyle patterns and risk factor profiles. Consequently, the observed threshold differences should reflect the combined influence of multiple population-specific factors rather than isolated ethnic effects. Third, the inherent biases associated with retrospective studies may affect the interpretation of our results. While we adjusted for known confounders, residual confounding may persist due to unmeasured variables that differ between populations, such as detailed dietary composition, physical activity patterns, socioeconomic factors, and healthcare access. Additionally, differences in laboratory standards and diagnostic practices between cohorts may contribute to some observed variations despite our efforts to standardize definitions. Fourth, we relied only on baseline AIP values to predict diabetes risk, and we could not assess the impact of AIP changes over time on risk prediction. Fifth, the study includes different population-specific backgrounds and lifestyles in China and Japan, which could lead to physiological differences among populations. Therefore, generalizing our findings from the Chinese to the Japanese cohort should be done cautiously. Sixth, reliance on initially self-reported diabetes diagnosis introduces the possibility of ascertainment bias. Differences between Chinese and Japanese healthcare systems, including access to medical resources, routine screening practices, and application of diagnostic standards, may lead to systematic differences in diabetes detection rates that could be misinterpreted as population-specific risk patterns. While we employed standardized follow-up assessments and uniform diagnostic criteria (American Diabetes Association standards) and adjusted for socioeconomic and healthcare access factors in multivariate analyses, the influence of diagnostic practice variations cannot be entirely eliminated. In particular, Japan’s higher healthcare accessibility and routine health checks may result in higher early diabetes detection rates compared to China, which might partially explain the threshold effect differences we observed. Seventh, this study relies on secondary analysis of two independent cohorts with different data collection periods and potentially different laboratory standards. While standardized definitions and robust statistical methods were employed, we acknowledge the inherent limitations in cross-population comparisons using retrospectively collected data. Differences in laboratory assays, measurement protocols, and other unmeasured factors may influence the absolute values of the identified thresholds, though the consistent association pattern supports the biological relevance of AIP across both populations. Eighth, a primary limitation of our study is the substantial proportion of missing data, particularly for AST (50.656% missing) and lifestyle factors (63.420% missing). While multiple imputation is a recommended approach for handling missing data, its reliability may decrease with higher missing rates. To mitigate concerns, we conducted sensitivity analyses using alternative imputation approaches. The consistency of our findings across these different analytical strategies suggests a degree of robustness in our results. However, the high proportion of missing data introduces uncertainty that cannot be fully eliminated through statistical methods alone. Future studies should prioritize more complete data collection, particularly for important clinical parameters and lifestyle factors. Despite these limitations, we believe our findings provide valuable insights into population-specific relationships between AIP and T2D risk, though they should be interpreted with appropriate caution. Ninth, the differences in mediation proportions between Chinese (39.84%) and Japanese (27.11%) populations could be influenced by measurement variability, unmeasured confounding factors, or inherent baseline differences between cohorts, rather than representing genuine population-specific biological pathways. Without longitudinal data tracking changes in AIP, BMI, and diabetes development over time, our mediation analysis should be considered exploratory and hypothesis-generating rather than conclusive. Our findings highlight several important directions for future research. (1) Prospective cohort studies with longitudinal assessments of AIP, BMI, and glycemic parameters are needed to establish the temporal sequence necessary for confirming the proposed mediation pathways. Such studies should incorporate repeated measurements over time to track how changes in AIP relate to subsequent changes in BMI and diabetes risk. This longitudinal design can address the inherent bias of cross-sectional mediation analysis. (2). Studies specifically designed to compare these relationships across well-characterized Asian populations would help determine whether our observed population differences reflect genuine biological variation or methodological artifacts. Such research should include a comprehensive assessment of potential mediators and confounders, including detailed measures of body composition (beyond BMI), dietary patterns, physical activity, and genetic factors. Following Yaghootkar et al.‘s research methodology[59], these studies should explore how ethnic differences in adipose tissue expansion capacity and fat storage efficiency influence metabolic risk. (3) Time-lagged analyses that can better establish temporal precedence would be valuable for clarifying the direction of causality in the relationships between lipid profiles, adiposity, and diabetes risk. These analyses should include multiple potential mediators to identify the most relevant pathways. Tenth, the difference in follow-up periods between the Chinese (maximum 7 years) and Japanese (maximum 12 years) cohorts may introduce systematic bias. Although Cox proportional hazards models account for varying follow-up times, and we standardized risk measurements using incidence rates per 1000 person-years, this design discrepancy may affect direct comparisons between populations. Specifically, the longer follow-up in the Japanese cohort might increase the cumulative opportunity for diabetes detection, potentially influencing incidence estimates. To mitigate this concern, we conducted sensitivity analyses restricting both cohorts to a common 7-year maximum follow-up period, demonstrating that our primary findings remained robust. Eleventh, an important limitation of our study is the inconsistent availability of anthropometric and biochemical measures between the Chinese and Japanese cohorts. While the Japanese dataset contained comprehensive measurements allowing calculation of WHR and FLI, the Chinese cohort lacked waist circumference measurements and components necessary for FLI calculation. This disparity prevented us from conducting comparative analyses of the mediating roles of hepatic steatosis and visceral adiposity across both populations. Consequently, our mechanistic insights regarding the differential contribution of fatty liver and central obesity to the AIP-diabetes relationship are limited to the Japanese population only. Future studies should aim to standardize data collection across diverse Asian populations to enable more robust cross-ethnic comparisons of these pathophysiological pathways. Finally, the dramatically different threshold values identified for diabetes risk between Chinese (AIP = 0.436) and Japanese (AIP=-0.449) populations require careful interpretation. These population-specific thresholds represent exploratory findings rather than established clinical cutpoints. The marked threshold difference likely reflects a combination of genuine biological and environmental variations rather than merely statistical artifacts. These thresholds lack external validation in independent populations and have not been tested in clinical settings. The different association patterns observed above and below thresholds in the two populations may reflect complex non-linear relationships between AIP and diabetes risk, as suggested by recent studies identifying non-linear associations between AIP and insulin resistance[13, 16]. To address these limitations, future research should include: (1) external validation in independent Chinese and Japanese cohorts; (2) prospective studies specifically designed to test the predictive value of these thresholds; (3) mechanistic studies examining the biological basis for these ethnic differences; and (4) clinical utility assessments to determine whether population-specific AIP thresholds improve risk stratification and treatment outcomes compared to conventional approaches. Additionally, moving these exploratory findings toward clinical utility will require the development of standardized AIP measurement protocols, integration with established risk factors, and cost-effectiveness analyses of implementing AIP-based screening strategies. Until such validation is complete, these population-specific thresholds should be interpreted appropriately.
In summary, this study confirms a significant positive association between AIP and diabetes risk in both Chinese and Japanese populations, and this association remains robust after adjusting for multiple confounding factors. We identified population-specific non-linear relationships and threshold effects, indicating that in the Chinese population, diabetes risk no longer increases significantly when AIP > 0.436, while in the Japanese population, significant associations are observed only when AIP>-0.449. Age, BMI, and systolic blood pressure significantly modify the relationship between AIP and diabetes, suggesting the importance of risk assessment and intervention strategies targeted at specific subgroups. Mediation analysis revealed the partial mediating role of BMI in the relationship between AIP and diabetes, with a higher proportion of mediation in the Chinese population (39.84%) compared to the Japanese population (27.11%). Furthermore, in supplementary analyses of the Japanese cohort, we found that hepatic steatosis (FLI mediating 23.78%) plays a more important role than visceral adiposity (WHR mediating 7.30%) in mediating the AIP-diabetes relationship, supporting the critical role of fatty liver in diabetes pathogenesis. These findings emphasize the necessity of developing population-specific risk thresholds and intervention strategies for different East Asian populations, considering the significant differences between the two populations in lifestyle, dietary patterns, and metabolic characteristics. Future research should focus on standardizing data collection to enable more robust cross-population comparisons and validating the clinical utility of these thresholds through prospective designs.
Comments (0)