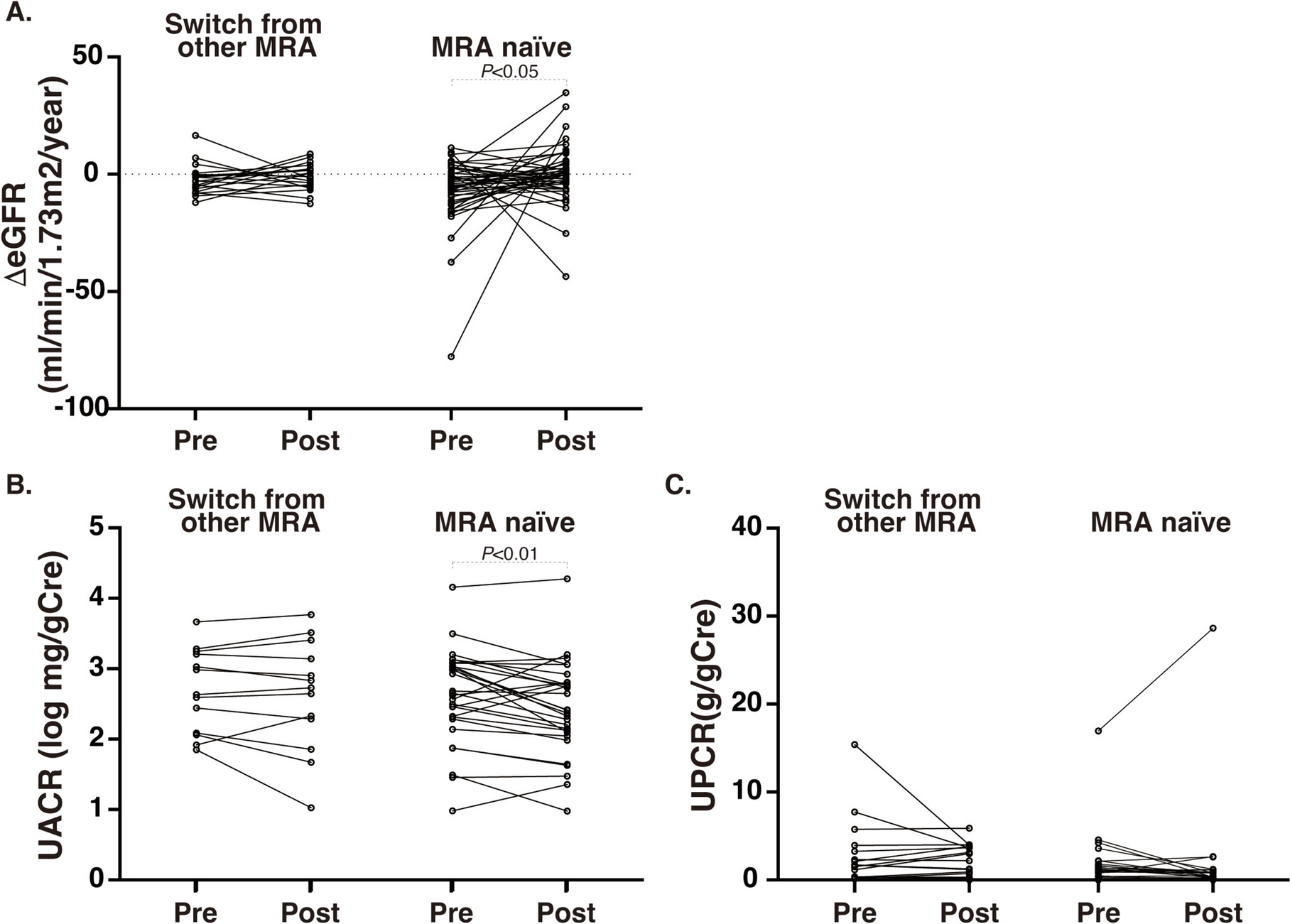
In this retrospective study, we evaluated the real-world clinical effectiveness of finerenone in patients with DKD. Our findings suggest that the addition of finerenone to comprehensive, evidence-based management significantly ameliorated the decline in eGFR. Interestingly, even in patients switched from other MRAs, finerenone appeared to preserve renal function based on eGFR slope analysis, despite no significant change in UACR.
The concept of MR antagonism as a therapeutic strategy for organ protection, particularly in cardiovascular disease, has been established for decades. The Randomized Aldactone Evaluation Study (RALES) demonstrated that spironolactone, beyond its diuretic effects, reduced all-cause mortality by 30% and significantly lowered cardiovascular mortality and hospitalization rates in patients with severe heart failure (left ventricular ejection fraction ≤ 35%, NYHA class III or IV) [18]. Subsequent studies confirmed the efficacy of second-generation MRA eplerenone in patients with both severe and moderate heart failure [19, 20]. More recently, third-generation MRA finerenone has also demonstrated cardiovascular benefit in trials such as FINEARTS-HF [21], FIGARO-DKD [9], and FIDELIO-DKD [10]. These results collectively support the role of MRAs in cardiovascular protection in patients with established heart disease, heart failure, and advanced DKD.
In contrast, renal outcomes associated with MRAs have historically been inconsistent. A large health insurance database analysis in Taiwan involving over 14,000 patients with CKD stages 3–4 revealed that spironolactone use was associated with a 34% reduction in ESKD incidence, albeit with increased hospitalizations due to hyperkalemia [22]. However, in pre-dialysis patients with stage 5 CKD, spironolactone use correlated with increased all-cause mortality and heart failure-related hospitalization [23]. In DKD populations specifically, while reductions in albuminuria have been consistently observed [12, 13, 24,25,26,27], robust evidence on hard renal outcomes was lacking until the publication of the FIGARO-DKD and FIDELIO-DKD trials. Notably, in Japan, eplerenone is contraindicated in patients with albuminuric nephropathy or advanced DKD. Furthermore, sub-analyses of the Japanese populations in the FIDELIO-DKD and FIGARO-DKD studies revealed unclear, and possibly adverse, renal effects [28]. Thus, in light of these uncertainties and limited clinical experience, real-world validation of finerenone’s efficacy in DKD is of significant importance.
Our analysis demonstrated a marked improvement in eGFR decline after finerenone administration (ΔeGFRprewhole: −7.3 ± 20.8 vs. ΔeGFRpostwhole: −0.5 ± 12.3 ml/min/1.73 m2/year, P = 0.010). A similar trend was observed when comparing ΔeGFR over the year prior to finerenone to that in the post-treatment period of ≥6 months (ΔeGFRpre1year vs. ΔeGFRpost6M~), with accompanying reductions in UACR. As shown in Table 1, the majority of patients receiving finerenone were already on SGLT2 inhibitors, and over half were treated with GLP-1 receptor agonists. The combination of SGLT2 inhibitor, GLP-1RA, and finerenone has been hypothesized to reduce kidney-related events by up to 58% [29]. While our study is a single-center, observational analysis and not conclusive, it provides strong support for current evidence-based, intensive DKD management strategies incorporating finerenone.
Interestingly, BMI was significantly reduced during the post-finerenone period, particularly in the MRA-naïve group. However, we do not consider this reduction to reflect a direct metabolic effect of finerenone. Rather, we suspect that the observed change may be due to hemodynamic effects, such as improved management of fluid overload. Supporting this notion, the FINEARTS-HF trial clearly demonstrated that finerenone exerted beneficial effects in patients with heart failure and mildly reduced or preserved ejection fraction [21], highlighting its impact on fluid regulation. Alternatively, renal protection by finerenone with UACR suppression, may have contributed to more appropriate volume management. Unfortunately, body fluid composition was not assessed in our study, and further investigations are warranted to clarify this mechanism.
Hyperkalemia is a common and serious concern in MRA therapy. In our cohort, no hyperkalemic crises were observed. Approximately 10% of patients were concurrently prescribed potassium binders such as sodium zirconium cyclosilicate or sodium polystyrene sulfonate to prevent hyperkalemia. In the FIDELIO-DKD trial, which enrolled high-risk patients (mean eGFR 44.3 ml/min/1.73 m2; median UACR 852 mg/g), 0.8% of finerenone -treated patients experienced serum potassium ≥6.0 mmol/L, compared to 0.2% in the placebo group [10], with minimal increases in acute kidney injury (AKI; 0.3% vs. 0.2%). In comparison, spironolactone-treated heart failure patients (mean age 73.2 years; mean eGFR 61.8 ml/min/1.73 m2; 46.6% with diabetes) experienced hyperkalemia and AKI rates of 2.9 and 10.1 per 1000 person-months, respectively, when co-administered with loop diuretics [30]. In FINEARTS-HF (mean eGFR 61.9 ml/min/1.73 m2), the incidence of hyperkalemia (>6.0 mmol/L) and serum creatinine ≥3.0 mg/dL in the finerenone group were 2.0% and 3.0%, respectively, during a median 32-month follow-up [21]. These findings suggest that finerenone may pose a lower risk of hyperkalemia and AKI compared to spironolactone.
Switching from another MRA to finerenone appeared to reveal a potentially distinct renal effect profile. Although our analysis did not reach statistical significance, switching to finerenone was associated with a trend toward renal protection, as reflected by the eGFR slope. The absence of a significant effect may be attributable to the limited duration of observation and the small number of patients with prior MRA use. Finerenone is the only MRA with clearly demonstrated efficacy in DKD through large-scale clinical trials. Importantly, each MRA exhibits distinct pharmacological characteristics [16]. Spironolactone, a steroidal MRA, has a long half-life (>20 h) and multiple active metabolites that also bind androgen and progesterone receptors. In contrast, finerenone is a non-steroidal MRA with a short half-life (2–3 h), no active metabolites, and no affinity for other steroid hormone receptors. Furthermore, in rodents, spironolactone accumulates in the kidney at sixfold higher concentrations than in the heart, while finerenone shows similar distribution in both organs [16]. These properties—short half-life, absence of active metabolites, and balanced tissue distribution—may make finerenone preferable in DKD patients at risk for acute kidney injury. Esaxerenone is another non-steroidal MRA with a receptor-binding profile similar to finerenone. However, it is primarily an antihypertensive agent, reducing systolic blood pressure by approximately 10 mmHg and exhibiting a prolonged half-life (19–25 h) [15]. Although its anti-albuminuric and antihypertensive effects are established, its long-term renoprotective potential remains speculative and likely differs qualitatively from that of finerenone. The difference of outcome after finerenone in blood pressure and BMI with or without prior MRAs should be not the direct influence of MRA; rather, prior MRA use group were much intensively monitored all biological parameters when compared to those of without.
There are several limitations to this study. First, it was a retrospective, single-center analysis with a small sample size. Given that finerenone was often initiated in patients already exhibiting progressive DKD, generalizing these findings to milder cases with normo- or microalbuminuria and preserved renal function may be inappropriate. Our sample size was also insufficient for robust subgroup analysis. Nonetheless, a key strength of our cohort is that most patients were already on SGLT2 inhibitors—unlike the FIGARO-DKD and FIDELIO-DKD trials, where concomitant use was limited. Additionally, the analysis of patients switched from other MRAs to finerenone offers novel insights into finerenone’s distinct renal effects.


Comments (0)