3DMax™ Mesh and 3DMax™ Light Mesh are standard (heavy)weight and lightweight versions of the same three-dimensional anatomically formed mesh, both used for inguinal hernia repair. Lighter-weight surgical mesh options were developed with the intention to reduce scar tissue, foreign body reaction and sensation, and chronic postoperative inguinal pain that can occur when implanting surgical mesh [7]. However, there is no specific delineation between heavy- and lightweight materials, and, until recently, there was limited evidence to compare outcomes, especially for laparoscopic repair and long-term results [7]. The current study found no significant differences in univariate analyses between comparable heavy- and lightweight meshes for short-term outcomes (i.e., interoperative complications, general complications, postoperative complications, complication-related reoperations), nor in terms of 1‑year outcomes including recurrence, trocar hernia, secondary hemorrhage, seroma, and infection. While heavyweight mesh was associated with significantly higher pain at rest and pain upon exertion at 1 year versus lightweight mesh, this only tended to be the case for pain requiring treatment at 1 year. However, the analyses could all only be conducted as univariate tests, i.e., without adjustment for confounders. The two main clinical outcomes (recurrence and pain) are assessed separately below.
Recurrence
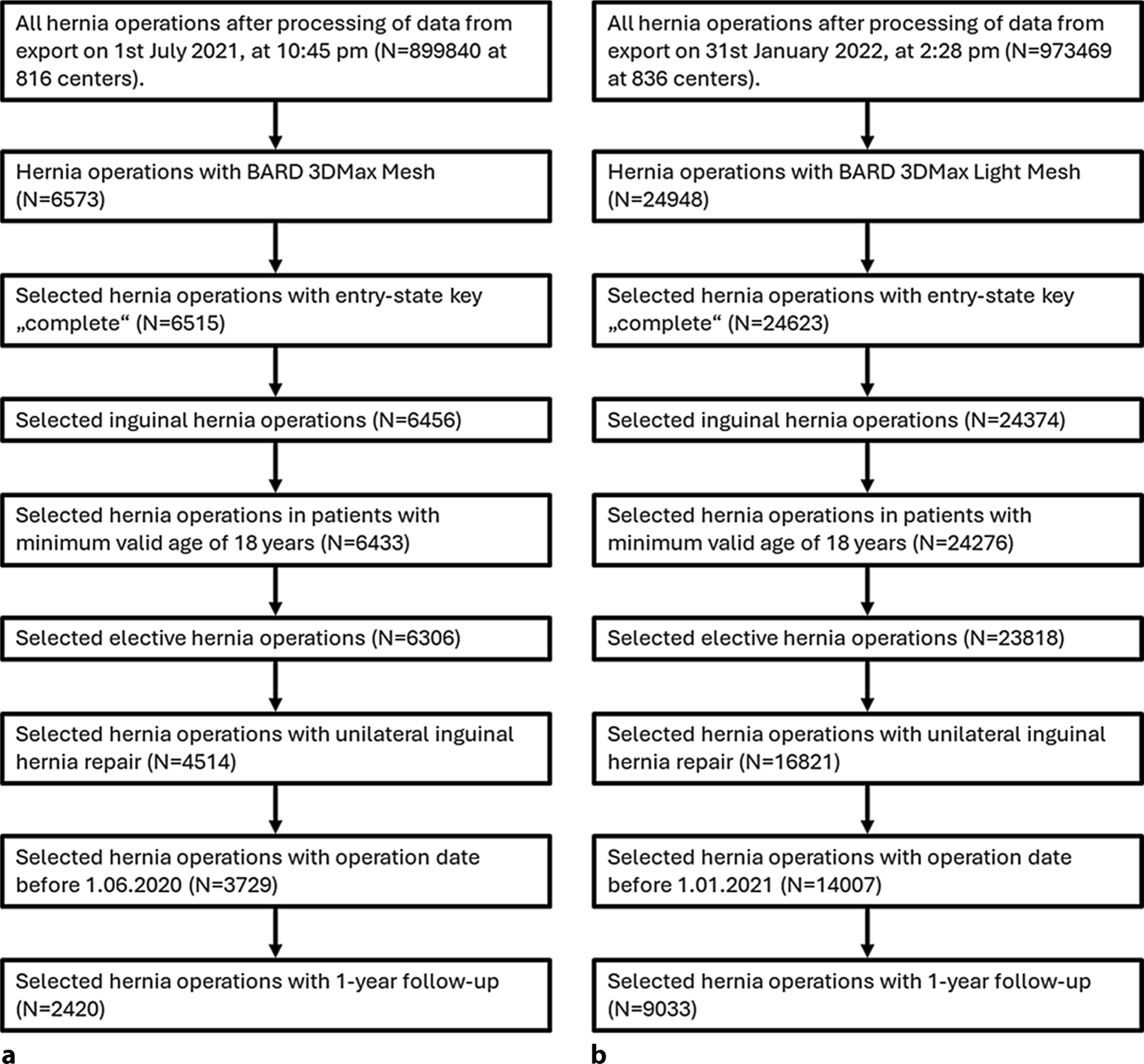
The comparison of Herniamed registry data for the standard/heavyweight and the lightweight meshes primarily used in laparoscopic repairs for 2420 and 9033 patients, respectively, showed similar recurrence outcomes (0.5% vs. 0.8%; P = 0.229) at 1‑year follow-up in unadjusted analyses. In comparison, registry data for more than 170,000 inguinal hernia repairs (suture, open, endoscopic) showed reoperation for recurrence rates of approximately 1.5% at 1 year, with 10.9% of patients requiring reoperation for recurrence over time [13].
Consistent with the current study, an analysis of more than 76,000 open inguinal hernia repairs in the Swedish Hernia Register reported no significant difference in recurrence between heavy- and lightweight polypropylene meshes throughout a median of 6 to 7 years follow-up, with an overall cumulative incidence of 2.2% for reoperation for recurrence [14]. Likewise, a randomized Swedish study found no significant difference in patient-reported recurrence at 9 to 12 years after open inguinal hernia repair with heavy- or lightweight flat polypropylene mesh (5.8% vs. 2.1%) [15].
However, an earlier analysis by Melkmichel et al. for more than 13,800 patients with laparoscopic totally extraperitoneal (TEP) repair from the Swedish Hernia Register showed a statistically significant difference in reoperation for recurrence between mesh weights, favoring heavyweight mesh (4.0% vs. 3.2%) throughout a median 6.1 years of follow-up, which was more apparent for direct and larger (> 3 cm) hernias [16]. Similarly, a meta-analysis of 12 randomized controlled trials (RCTs) with follow-up from 3 to 60 months for 2909 patients with laparo-/endoscopic surgery for uncomplicated inguinal hernias showed that use of heavyweight mesh significantly decreased the risk of hernia recurrence, especially in non-fixated direct or large inguinal hernia repairs [17]. However, there was no significant difference in terms of recurrence between mesh weights in subgroup comparisons of direct hernia repairs, indirect hernia repairs, or repairs with mesh fixation [17].
The variation in evidence for recurrence may be explained by different follow-up times, operative approaches (e.g., open versus laparoscopic), patient populations, and definitions of recurrence. A systematic review was conducted to support the 2023 update to the International HerniaSurge guidelines, which analyzed the evidence for mesh type and characteristics most suitable for open and laparo-/endoscopic repair. For open repairs, the evidence suggests there was no effect of mesh weight on recurrence, except for partially absorbable lightweight mesh, which showed higher recurrence rates compared to permanent light- or heavyweight mesh [7]. For laparo-/endoscopic repair, the risk of recurrence was not affected by mesh weight for small and lateral defects, though heavyweight mesh is recommended to reduce the risk of recurrence for large and direct hernias [7].
Pain
While pain upon exertion (10.6% vs. 9.2%; P = 0.035) and at rest (5.8% vs. 4.6%; P = 0.014) was significantly higher for the heavyweight mesh compared to the lightweight mesh in unadjusted analyses, there was no clear significant difference in pain requiring treatment (3.6% vs. 2.9%; P = 0.095), although it also tended to be higher for the heavyweight mesh compared to the lightweight mesh. It is challenging to compare pain outcomes to the standard of care since the reporting methods and timeframes in the literature vary substantially. For example, patient-reported pain outcomes at 9 to 12 years after surgery from the Rutegard et al. publication described pain that was present but easily ignored (14.9% heavyweight vs. 5.3% lightweight) and pain that was present that cannot be ignored (5.8% vs. 3.3%, respectively) among other pain outcomes; however, the length of time and descriptions of pain are quite different from those reported via Herniamed [15]. A meta-analysis by Konig et al. evaluated chronic pain (defined as pain persisting for longer than 3 months) in patients with TEP vs. Lichtenstein inguinal hernia repair, reporting rates of 12.4 and 16.8%, respectively [18]. The most relevant comparison may be from the Herniamed registry, where an analysis of data of more than 20,000 patients with elective primary unilateral inguinal hernia repair using the TAPP technique reported rates for pain at rest (4%–5%), pain upon exertion (8%–10%), and pain requiring treatment (2%–3%) [19]. These rates are generally in line with the rates reported in this publication for 3DMax™ and 3DMax™ Light meshes, which in many cases (70–80%) were placed using the TAPP technique, although various other techniques were also used, so the datasets are not directly comparable.
The complexity of evaluating pain outcomes across datasets was apparent in the analysis by Niebuhr et al., who reported myriad factors (e.g., age, preoperative pain, hernia defect size, body mass index [BMI], mesh size, other postoperative complications, fixation technique) that were significantly associated with pain rates in their analysis [19]. In the current study, there was an apparent higher percentage of patients without fixation for the heavyweight 3DMax™ (83.6%) compared to lightweight 3DMax™ Light (60.5%), yet pain at rest and upon exertion was significantly lower for the lightweight mesh, with only slight differences in pain requiring treatment. Further analysis including this confounder—among others—is necessary, given that fixation is known to impact pain. One study reported a statistically significant difference in pain impacting daily activities (12.0% vs. 26.4% reported no pain) and perception of foreign material in the groin (4.5% vs. 15.4%) favoring lightweight mesh [15]. All other pain, discomfort, or sensation measures showed no significant differences between mesh weight groups [15]. However, these results for open inguinal repair and/or flat mesh may not be generalizable to laparoscopic surgery using anatomical mesh.
A meta-analysis of 12 RCTs with follow-up from 3 to 60 months for 2909 patients with laparo-/endoscopic surgery for uncomplicated inguinal found no significant differences in the risk of any pain or severe pain or foreign body sensation between mesh weights, although the ability to evaluate pain outcomes was challenged by a lack of evidence [17]. A systematic review to support the 2023 update to the international HerniaSurge guidelines analyzed the evidence for mesh type/characteristics most suitable for open and laparo-/endoscopic repair as well as recurrence and chronic postoperative pain for each [7]. For open repair, the evidence suggests an increased risk of chronic pain and foreign body sensation with heavy- versus lightweight mesh [7]. For laparo-/endoscopic repair, the occurrence of chronic pain was not affected by mesh weight. [7].
Limitations
There are some limitations to the Herniamed registry data analysis reported herein. The datasets were collected from different time periods for the heavy- mesh and lightweight meshes. All patients were included in this investigation without adjusting for confounders, so there is variability in patient demographics and operative details. Further, the analysis in this paper included multiple surgical techniques (open and laparoscopic/endoscopic) and all hernia sizes, which can impact recurrence and pain. Future studies should assess the interaction between mesh weight and these factors. There is also a need to consider longer-term outcomes beyond 1 year, although that is compensated by considering the substantial published literature on both 3DMax™ Mesh and 3DMax™ Light Mesh since their time on the market, with recurrence data through at least 5 years for each.
In light of the surgical mesh options available in terms of mesh weight, shape, and other characteristics as well as the potential impact of numerous variables on clinical outcomes [19] and the difficulties associated with generalizing the evidence for some heavy- or lightweight mesh to other meshes on the market [7], mesh selection based on these various mesh, patient, and surgical parameters is important [1]. As such, it is beneficial to have options like the standard (heavy)weight, midweight, and lightweight versions of 3DMax™ available for surgeon preference and clinical need.
Missing 1‑year follow-up data for a relevant proportion of patients is another limitation. However, calculation of standardized differences between patients with and without follow-up does not point to any selection bias.





Comments (0)