Role of stromal area and tumor:stroma ratio in predicting response to neoadjuvant chemoradiotherapy in rectal cancer patients
Background
Neoadjuvant chemoradiotherapy (nCRT) improves outcomes in locally advanced rectal cancer (LARC). However, the response varies, thus necessitating predictive markers.
Methods
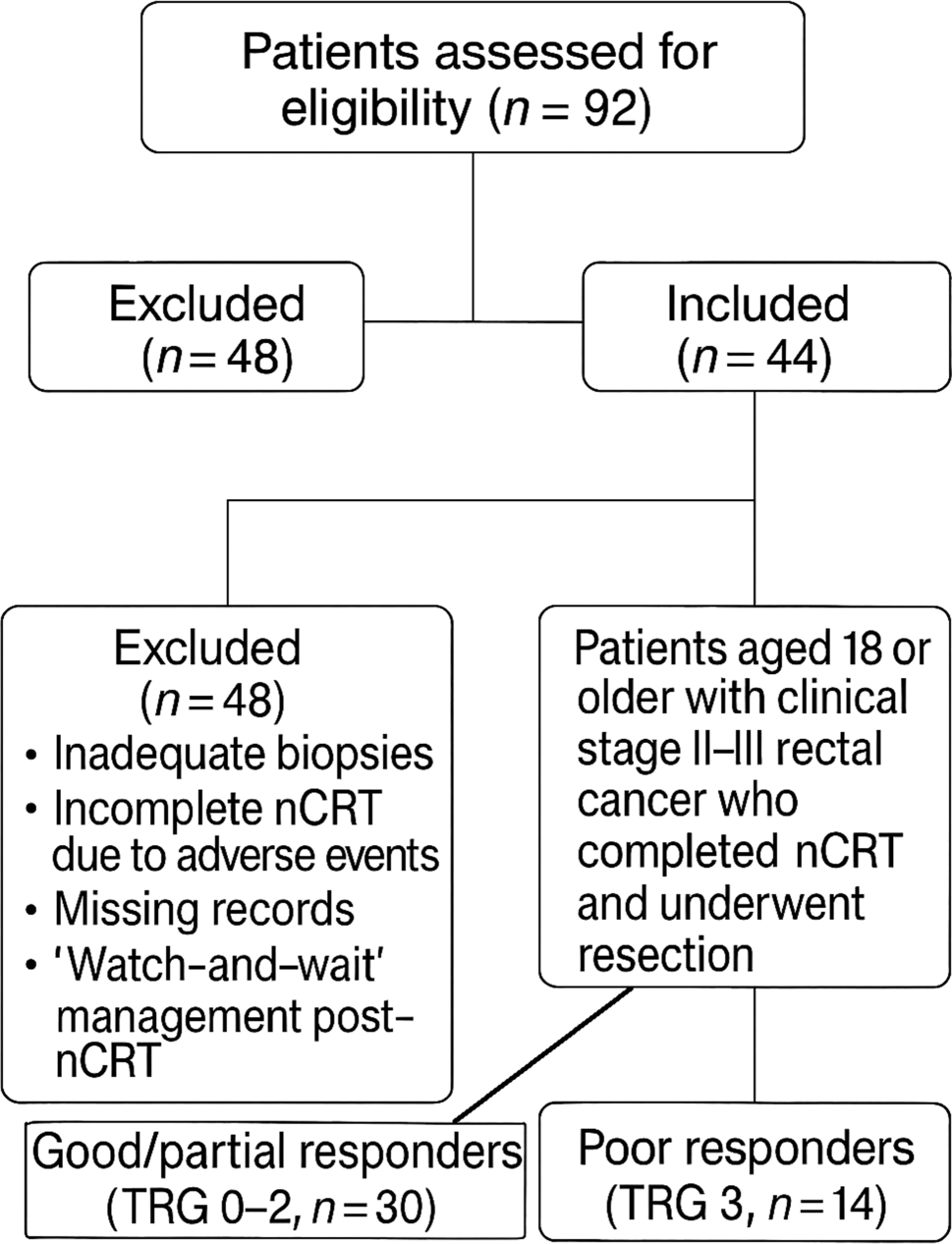
We analyzed 44 LARC patients treated with nCRT followed by surgical resection. Pretreatment biopsies were evaluated for the tumor:stroma ratio (TSR) and stromal area using digital image analysis by two pathologists. Pathological response was graded with the College of American Pathologists Tumor Regression Grade (CAP-TRG).
Results
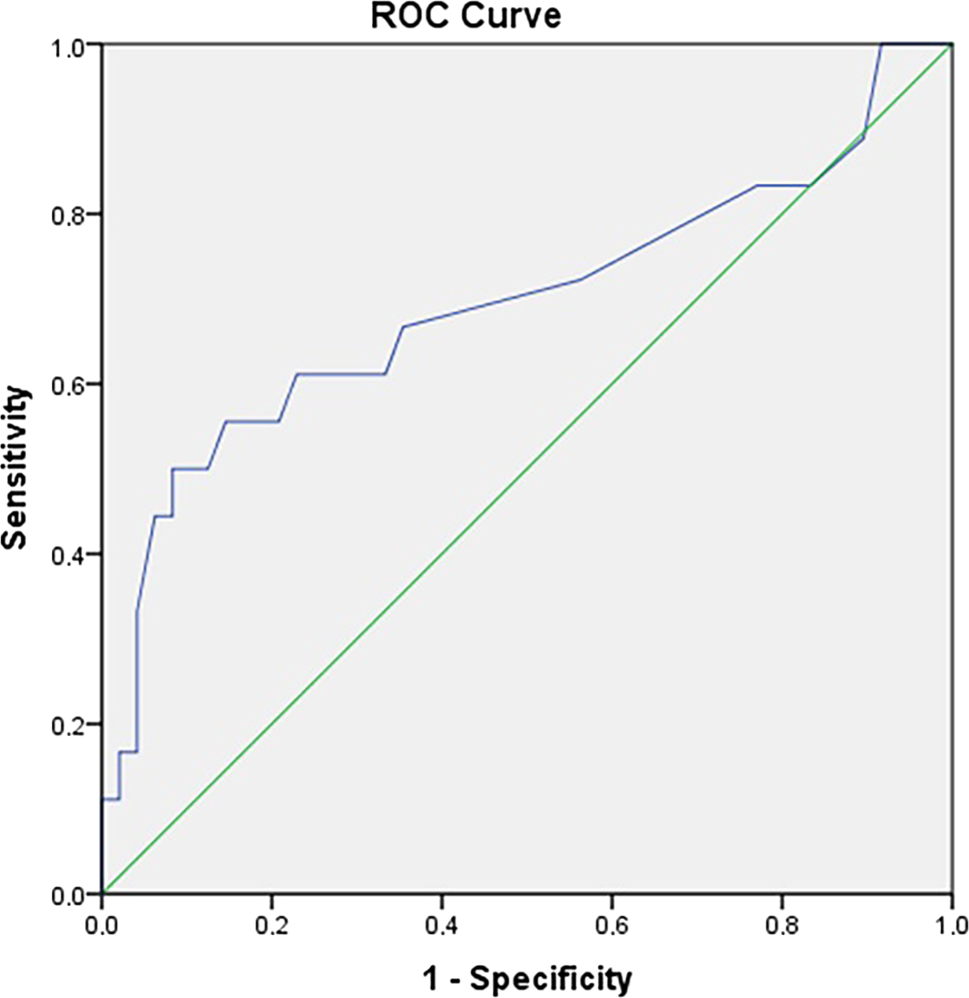
Good/partial responders (TRG 0–2) comprised 68.2% of the cohort. Median stromal area was lower in good/partial responders (2.5 mio. px2 vs. 3.3 mio. px2; P = 0.006). Median TSR was higher in good/partial responders (0.85 vs. 0.38) but not significantly (P = 0.137). Receiver operating curve (ROC) analysis identified a stromal area cut-off of 2.9 mio. px2 (area under the curve [AUC] 0.745, sensitivity 80.77%, specificity 64.29%; P = 0.009) for a poor response. Multivariate regression confirmed stromal area (odds ratio [OR] 2.14, 95% confidence interval [CI] 1.12–4.09; P = 0.021) and perineural invasion (OR 3.45, 95% CI 1.33–8.94; P = 0.010) as independent predictors.
Conclusion
Higher stromal area predicts a poorer nCRT response in LARC, while TSR trends toward significance. Stromal area may guide personalized treatment, pending larger cohort validation and practical implementation in clinical settings.





Comments (0)