This study was approved by the Tata Memorial Hospital’s Institutional Ethics Committee and written informed consent was obtained from all subjects participating in the trial. The trial was registered prior to patient enrolment at Clinical Trial Registry of India (CTRI/2021/02/031151, registered on 9th February 2021).
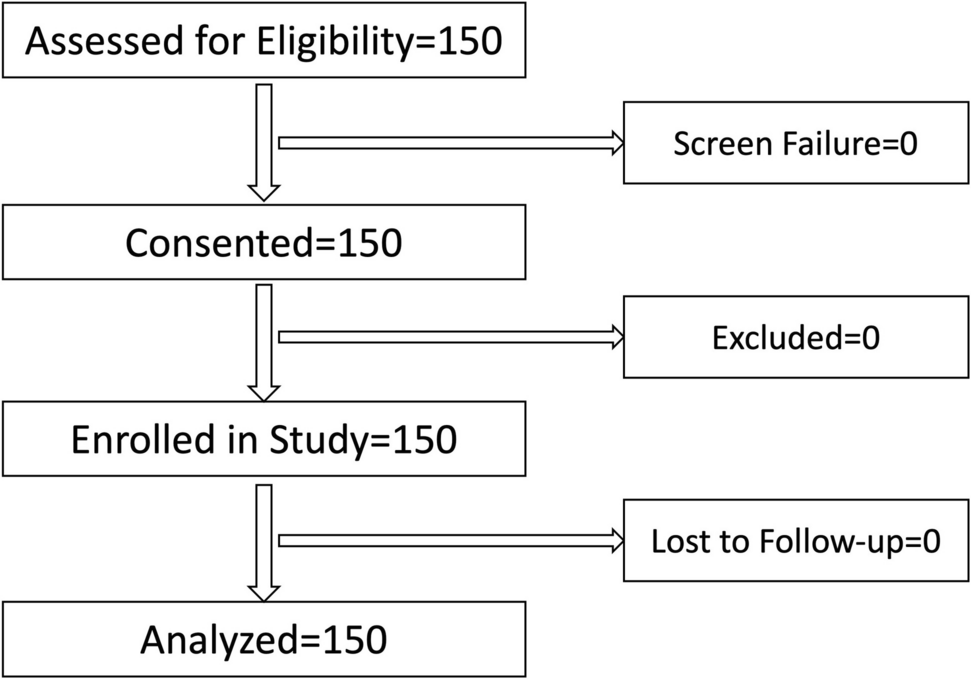
Thirty ERAS elements were chosen based on a combination of internationally recognized ERAS guidelines for major abdominal surgeries and institution-specific ERAS protocols for CRS-HIPEC. These elements were selected a priori by a multidisciplinary team, including anaesthesiologists, surgeons, and critical care physicians, to reflect the most relevant components. A total 150 patients were included consecutively who were undergoing CRS-HIPEC. The primary objective to study the association between compliance to the ERAS components and postoperative outcomes defined by Clavien-Dindo classification [14] and secondary objectives were to study the association of the compliance of ERAS components with length of hospital stay, readmissions within 30 days of the surgery and delay in RIOT.
This study was conducted at a tertiary cancer care center where ERAS pathways are well established. The perioperative team, consisting of anesthesiologists, critical care physicians, surgeons, physiotherapist, nutritionist, and nursing staff, are all trained and actively involved in adhering to the ERAS protocols. These pathways are integrated into routine clinical practice to optimize patient outcomes. All consecutive patients aged between 18 and 80 years who were planned for CRS-HIPEC between the period May 2021 and August 2023 were screened for inclusion into the study. All patients were explained in detail about the ERAS protocols and an informed consent is obtained from them as per their preferred language (English/Hindi/Marathi).
In this study, no interventions were done except for the collection of data of the standard of care. Data was collected in preoperative period, intraoperative period, and postoperative period. In the preoperative period, demographic details such as age, gender, body mass index, and preoperative parameters and assessment including ASA grading, comorbidities, prehabilitation, namely cessation of smoking and alcohol, chest and physical physiotherapy started or not, anemia correction, nutritional optimization, fasting duration, thromboprophylaxis, carbohydrate loading, and skin preparation done or not. In the intraoperative period, analgesia technique, techniques and goals of fluid therapy, and temperature management during CRS and HIPEC phases. In the postoperative period, patient’s physiological stability at the time of postoperative transfer to intensive care unit (ICU) or ward, elective ventilation, pain management, postoperative mobilization, intravenous fluid therapy, removal of drains, type and days of feeding initiation, thromboprophylaxis, and recovery of bowel functions were noted. Postoperative complications as per Clavien-Dindo classification, in hospital mortality, and 30 days all-cause mortality were also noted. All patients were followed up for 30 days post-surgery for re-admissions and delays in RIOT. In an event of lost-to-follow up, attempts were made to contact the patient or family. All the data was collected by a dedicated ERAS team using a separate case record form designed for this study and the hospital electronic medical records for analysis. We found the appropriate cut off value for compliance percentage to be 71.6% (area under curve [AUC] 0.82; p value < 0.001) using compliance percentage as a continuous variable (test variable) and postoperative complications (state variable). Based on the cut off value, the patients were divided into high compliance group (> 71.6%) and low compliance group (< 71.6%).
Statistical Analysis
Descriptive statistics were used to summarize baseline characteristics, with continuous variables presented as mean ± standard deviation (SD) and categorical variables as frequencies and percentages. The normality of data was assessed using the Shapiro–Wilk test. For inferential analysis, Pearson correlation was used to assess the linear relationship between the peritoneal carcinomatosis index (PCI) and both postoperative complications and ERAS compliance percentage and to evaluate the relationship between ERAS compliance percentage, postoperative complications (Clavien-Dindo grading), hospital stay, readmissions, and RIOT. Receiver-operating characteristic (ROC) curve and Youden index were used to establish the cut-off values of compliance percentage and grouped the data to high compliance percentage and low compliance percentage. Chi-square analysis was used to assess associations between grouped compliance percentages (high vs. low) and outcome variables such as postoperative complications, hospital stay, and delays in RIOT. Logistic regression analysis was done to assess the relation between ERAS compliance percentage and postoperative complications and length of hospital stay. All statistical analyses were performed using Statistical Package for Social Sciences (SPSS) software version 25 (SPSS 25, IBM Inc., Chicago, IL, USA), with a significance level of p < 0.05.

Comments (0)