Study area, period, and setting
A hospital-based, retrospective cohort study was conducted from September 2018 to August 2023 at the ambulatory clinic of the University of Gondar Comprehensive and Specialized Hospital (UOG-CSH). The UOG-CSH is a tertiary facility located in the Central Gondar Zone of the Amhara Regional State, approximately 750 km from Addis Ababa. The hospital provides both inpatient and outpatient services to over 7 million people in urban and rural areas throughout the central Gondar Administrative Zone. It has more than 500 beds available for inpatient care in its internal medicine, pediatrics, surgery, gynecology, and obstetrics wards. Additionally, each department includes outpatient departments (OPD) where ambulatory care is offered to patients with new or chronic conditions, such as HF. According to health management information system (HMIS) data, chronic heart failure is the second most prevalent cardiovascular disease in hospitals. Currently, over 2,750 patients with CHF receive outpatient medical care services in the Northwest Ethiopia area.
Population
The source population included all adult patients with HFrEF who had follow-up at the ambulatory clinic of UOG-CSH, while the study population comprised patients with HFrEF who met the specified inclusion criteria and attended the ambulatory clinic of UOG-CSH for follow-up during the study period.
Eligibility criteriaInclusion criteria
Patients ≥ 18 years old, whose baseline information was documented in their medical chart,
Ambulatory HFrEF patients who had a follow-up period of at least 6 months [19].
Patients with an EF of ≤ 40% [12] based on a recent echocardiogram performed within the last 2 years, and
patients willing to participate in the study, were included in the study.
Exclusion criteria
Sample size determination and sampling technique
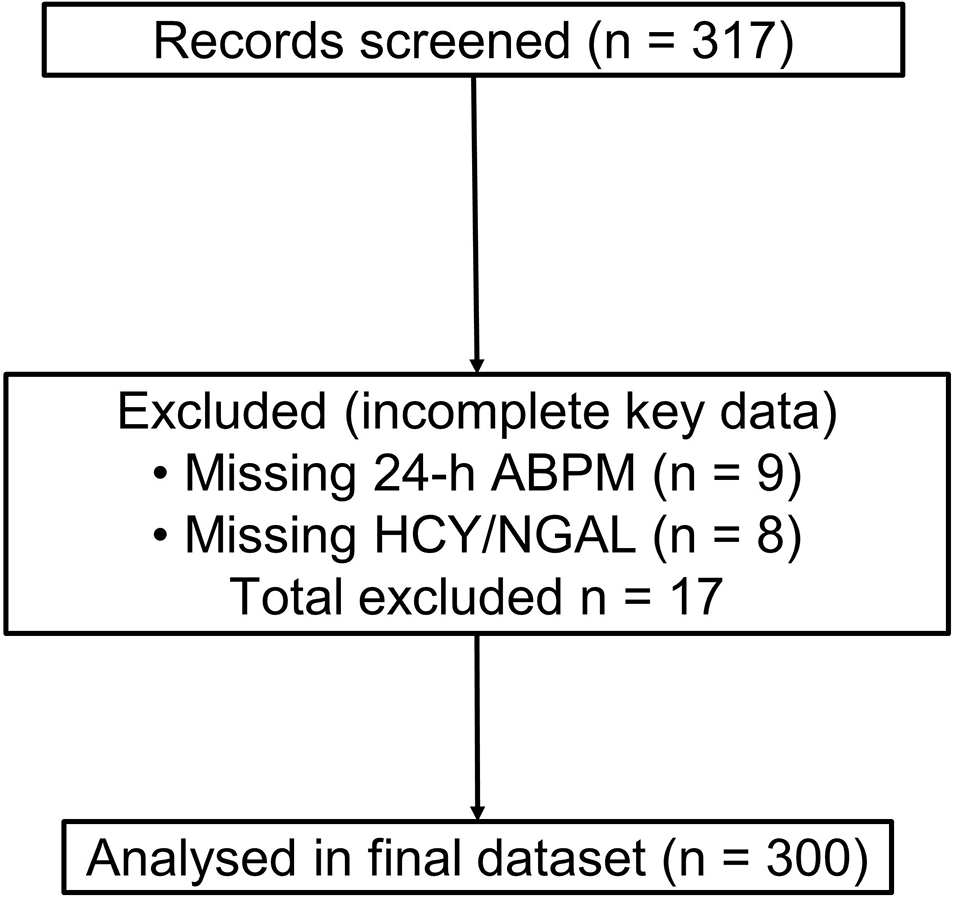
The number of patients needed for the study was calculated using a formula that considers a 95% confidence level, a 5% margin of error, and an estimated 37.6% use of guideline-recommended BB based on a previous study at Tikur Anbessa Specialized Hospital [20], resulting as follows:
$$\left(\text\right)=\frac=\frac=362$$
Adding 17% non-respondents, the final sample size was 423 individuals.
Where:
Zα/2 = 1.96, the standard score (critical value) corresponding to a 95% CI
p = 0.38, represents the estimated percentage of patients with HF who used evidence-based BBs
q = 0.62, proportion of (1-p)
d = 5%, the proportion of sampling error
n = sample size.
A systematic random sampling technique was used to select 423 participants from a source population of 1,750 patients with HFrEF attending follow-up over 4 months. The sampling fraction (K) was calculated as:
Then, the first participant was randomly selected by lottery (number 3), and every 4 th patient thereafter was included.
For the qualitative study, nine physicians were purposively selected with maximum variation from the UOG-CSH for interviews.
Operational definitionsBeta-blockers are deemed to be "tolerated"
If the blood pressure is ≥ 90/60 mmHg, the heart rate is > 60 beats per minute, and there is no current evidence of bronchospasm. Otherwise, the BBs were considered to be"non-tolerated" [21, 22].
Appropriate dose titration of BBs
The time interval between the dose titrations will be ‘appropriate if the tolerated dose is timely titrated (every 2 to 4 weeks’ interval). However, the time for a dose titration was considered"inappropriate’ if the dose was not titrated within 2 to 4 weeks of the time interval [23].
Optimal dose of BBs
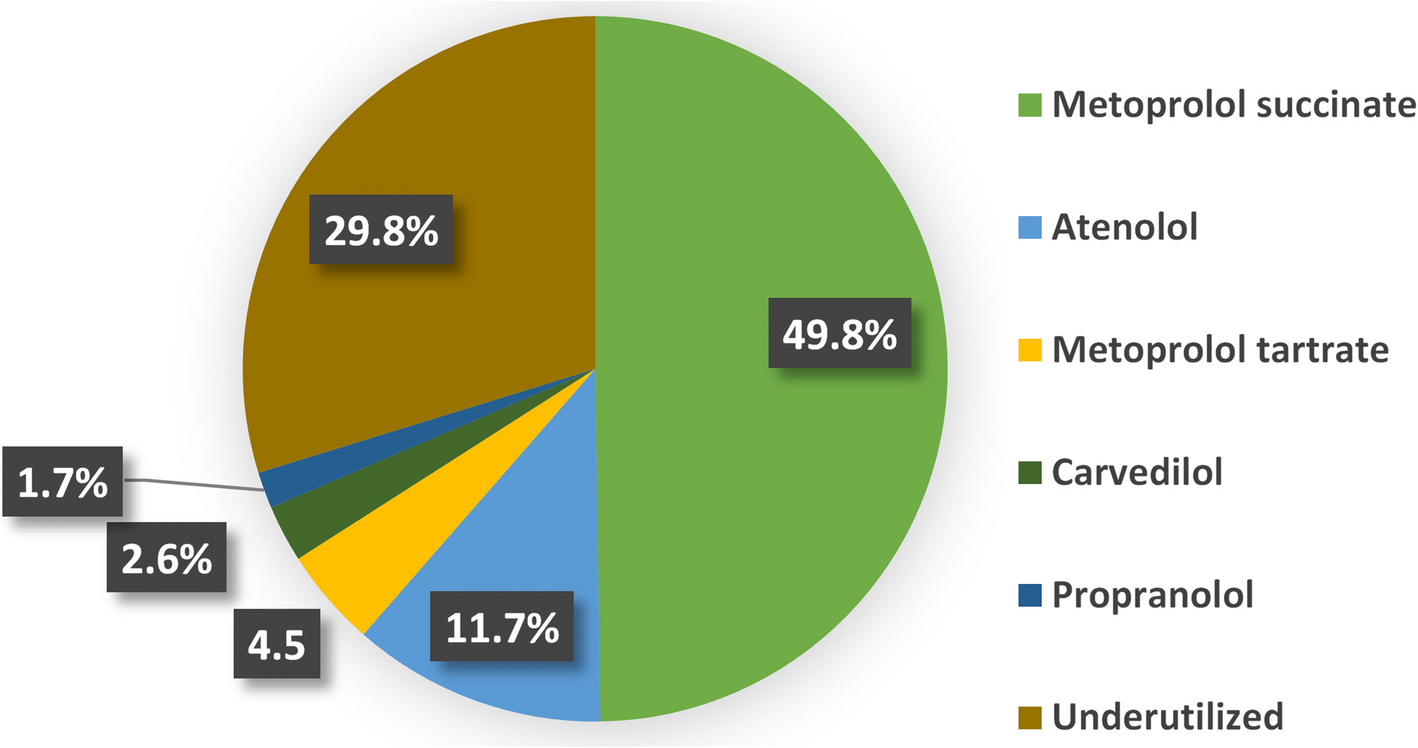
Based on the recommendations, it will be given at the recommended target dose or the maximum tolerable dose given for the patients. For metoprolol succinate, the optimal dose will be considered if the dose is 200 mg daily or a maximum tolerable dose, bisoprolol, 10 mg daily, or a maximum tolerable dose, 50 mg/day for Carvedilol [24].
Suboptimal dose of BBs
If the patient is taking any dose of BBs below the target dose in the absence of contraindications for up-titration [22].
Underutilized BBs
If not used by the patients in the absence of contraindications [11, 25].
The overall BB treatments are deemed to be'optimized'when the dose of BB is optimized through timely titration, and the patient tolerates the BBs [25, 26].
Data collection techniques and data quality control
A structured questionnaire was developed by reviewing similar studies [5, 12, 15, 27, 28]. The format included the sociodemographic, clinical, and treatment characteristics of the patients, which were gathered through standardized interview questionnaires. Clinical and treatment-related characteristics were obtained from the patient's medical records from September 2018 to August 2023. The questionnaire was pretested on 5% of participants (n = 21) at Felege Hiwot Comprehensive Specialized Hospital, Bahir Dar, using Cronbach’s alpha, yielding a reliability score of α = 0.835, indicating high internal consistency. Data were collected by three clinical pharmacists, under the supervision of an appointed supervisor from May 2023 to August 2023 G.C. (data collection period). All received two days of training on the study’s objectives, tools, ethics, and responsibilities. The principal investigator and supervisor reviewed data daily, making immediate corrections when needed.
The principal investigator collected the data for the qualitative portion of the study from August 1 to 31, 2023 G.C. Data was collected using a semi-structured, in-depth interview guide. Interviews were done by telephone call and audio recording (chosen time mostly on Saturday and Sunday) by the physicians. Data collection stopped once data redundancy occurred, whereby additional participants did not provide crucial new information [29, 30]. A topic guide was designed based on the specific objectives of the study (research question) and developed based on a review of relevant literature and international guidelines. The audio recordings in Amharic were transcribed verbatim into English to avoid loss of information. Every recorded interview was given a unique identification number. The security of the records was ensured by password protection, and the records can only be accessed by authorized users.
Data quality control and data analysis
Data collected via the Open Data Kit (ODK) Toolbox (version 2023.2.4) were analyzed in Excel and exported to SPSS version 27.0 for further analysis. Descriptive statistics were presented using narration, tables, and graphs. Before bi-variable and multivariable logistic regression, outliers and multicollinearity were assessed. Variance inflation factor (VIF) values were < 2.1 for BB utilization and < 1.4 for dose optimization, indicating no multi-collinearity.
A binary logistic regression analysis was performed using both bi-variable and multivariable approaches. Variables with p < 0.25 in the bi-variable analysis were included in the multivariable model to control for confounding. In the multivariable analysis, variables with p < 0.05 were considered statistically significant, and adjusted odds ratios (AOR) with 95% confidence intervals were reported. Model fit was supported by the Omnibus test (χ2 = 99.81, df = 14, p < 0.001 for utilization; χ2 = 43.34, df = 7, p < 0.001 for dose optimization), indicating significant improvement over the null model. The Hosmer–Lemeshow test confirmed a good model fit (p = 0.806 for utilization; p = 0.094 for dose optimization). Nagelkerke’s R2 showed that the models explained 30% and 37.4% of the variance in BB utilization and dose optimization, respectively.
In the qualitative portion of the study, the data were collected and analyzed manually following an inductive thematic analysis by the primary investigator as suggested by Ayton and Braun & Clarke [30, 31]. The audio data were first transcribed verbatim from Amharic into English. To achieve data immersion and familiarization, the transcripts were read multiple times to capture meaningful segments and grasp the essence of the content. Following familiarization, open coding was conducted by writing codes directly onto the transcripts or recording them in a separate document. After generating the initial codes, the researchers reviewed and grouped similar or related codes to form broader categories that reflected common ideas. These categories were then analyzed at a higher, more abstract level to develop overarching themes. Through this systematic process, open codes were organized into several categories, and categories were ultimately refined into key themes. Finally, the study team collaborated to review, discuss, and refine the categories and themes, reaching a consensus on the key themes that emerged from the data.
Ethical consideration and consent to participate
Ethical clearance was obtained from the Institutional Review Board (IRB) of the UOG, College of Medicine and Health Science (CMHS, as well as the Department of Clinical Pharmacy, before conducting the study with the approval number of SOPs/278/2023. The clinical directorate of the ambulatory clinic at UOG-CSH issued a letter of permission. Privacy and confidentiality were maintained during patient interviews and the review of patients'medical records. After explaining the study's purpose, verbal informed consent was secured from HF patients. For patients with hearing or speaking difficulties, verbal informed consent was obtained from the patient's caregivers. In the qualitative portion of the study, informed consent was obtained before telephone interviews. Physicians were requested to sign a consent form and return it to the data collector via email or text message. Password protection ensured the security of the records, allowing access solely to authorized users.




Comments (0)