
Remember me


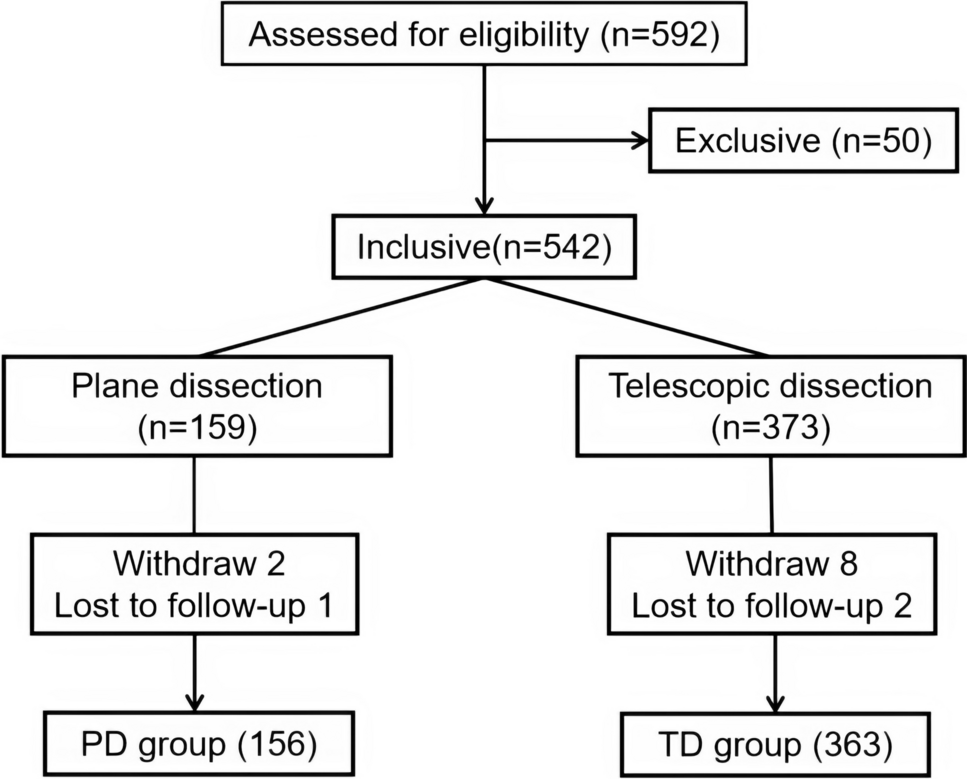

A retrospective analysis was conducted on the clinical data of patients undergoing TEP surgery at the department of surgery in our hospital. The study included two groups: the plane dissection group (PD group) and the telescopic dissection group (TD group). Inclusion Criteria: (1) Married patients older than 25 years; (2) Able to participate in reliable follow-up. Exclusion Criteria: (1) Old and frail patients unable to withstand general anesthesia; (2) Patients with severe cardiopulmonary, liver, or kidney dysfunction. (3) Patients with severe coagulation disorders; (4) Patients with a history of lower abdominal surgery; (5) Patients with a history of urinary system surgery; (6) Patients with incarcerated or strangulated hernia; (7) Patients with a large hernia sac that cannot be reduced; (8) Patients who withdraw from the study midway. Based on these criteria, a total of 519 cases were collected, including 156 in the PD group and 363 in the TD group. After 1:2 propensity score matching, 156 cases were successfully included in the PD group and 312 in the TD group (Fig. 1). Before matching, the PD group had a higher proportion of indirect hernias, while fewer direct hernias and type II hernias were observed. In contrast, the TD group had an older age. After matching, there were no statistically significant differences in clinical characteristics between the two groups (Table 1). The study was approved by the Ethics Committee of our Hospital, and all patients provided written informed consent before surgery.
Fig. 1
Flowchart of inclusions and exclusions of all participants in the study
Table 1 Clinical data and baseline characteristics of the two groupsSurgical techniquesPlane dissection procedureA small incision is made 2 cm above the umbilicus and then 1.5 cm laterally, through which the skin, subcutaneous tissue, and anterior rectus sheath (ARS) are excised to access the retromuscular space. (Fig. 2a). A 10 mm trocar is inserted through this incision to access the first surgical plane located between the rectus and posterior rectus sheath (PRS), establishing the initial working space. A 5 mm trocar is placed below the umbilicus, and another 5 mm trocar is positioned at the midpoint between the umbilicus and the pubic symphysis. Dissection continues along the surface of the PRS until it reaches the intersection with the transversalis fascia (i.e., the arcuate line). It then incised to enter the preperitoneal space, thus completing the first anatomical plane transition. The dissection is extended caudally into the same layer of the Retzius space, which constitutes the second surgical plane. Subsequently, the dissection is redirected laterally towards the groin area, freeing the Bogros space situated between the peritoneum and the deep layer of the preperitoneal fascia. This establishes the third surgical plane. Care must be taken to preserve the preperitoneal fatty tissue in order to avoid chronic pain caused by nerve irritation within the "pain triangle" due to the mesh. The hernia sac is then reduced. Femoral and direct hernias can be separated in the Retzius space, while direct hernias larger than 5 cm are sutured to the pubic ramus to prevent seroma formation. The reduction of an indirect hernia necessitates the incision of the internal spermatic fascia and meticulous dissection of the hernia sac from the spermatic vessels. These vessels should be stripped cranially at least 6 cm from the internal ring, and the vas deferens should be dissected until the obliterated umbilical artery is encountered. Finally, the interfoveolar ligament is incised to complete the second anatomical plane transition. This integrates the two distinct planes of the Retzius and Bogros spaces into a single large preperitoneal space, which accommodates the mesh effectively. A 3D mesh measuring 10.8 cm × 16 cm (Bard Davol Inc. Warwick, RI, 02886, USA) is placed without fixation in the created preperitoneal space to complete the preperitoneal hernia repair [11, 12]. The trocars are removed under direct vision, and the skin incisions are then sutured (see the Supplementary Video).
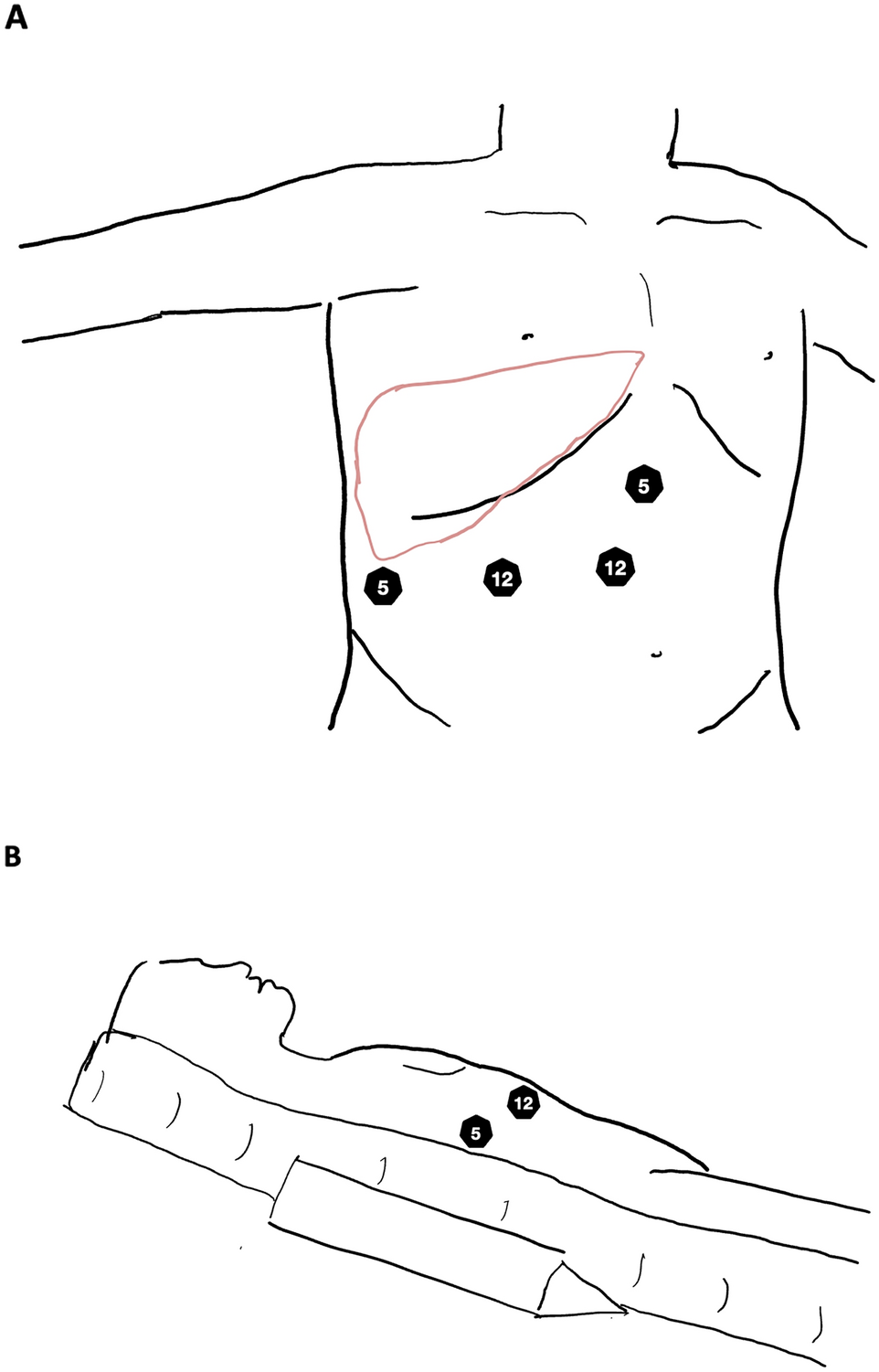
Fig. 2
Comparison of preperitoneal space dissection between the PD and TD groups. a Plane dissection: The retromuscular space was meticulously identified between the rectus and the PRS, followed by careful dissection along the PRS up to the arcuate line, where an incision was made to access the preperitoneal space. b Telescopic dissection: Blunt rod separation was performed forward, backward, and laterally along the PRS. Multiple “cellular” separation holes were observed, with some penetrating through the PRS into the preperitoneal space while others remained within the retromuscular space, resulting in minor bleeding from small blood vessels
Telescopic dissection procedureA small incision of approximately 1.0 cm is made below or beside the umbilicus, cutting through the linea alba or ARS. The rectus muscle is retracted to expose the space behind it. The telescope is then advanced along the PRS, breaking through the peritoneal fascia, and entering the preperitoneal space (Fig. 2b). The telescope is moved forward, backward, and laterally to separate and expand the preperitoneal working space. A 10 mm trocar is placed at the umbilical incision site, and two 5 mm trocars are inserted approximately one-third above and one-third below the midpoint between the umbilicus and the pubic symphysis. Like the PD group, dissection begins in the medial compartment (Retzius space), where direct and femoral hernias are easily identified and reduced. Subsequently, the lateral compartment (Bogros space) is separated, where an indirect hernia is often dissected and reduced. The remaining steps are essentially the same as those in the PD group described above.
Observation indicatorsThe main outcomes of the study were peritoneal injury, vascular injury, surgical visual field clarity, operative time, intraoperative blood loss, and postoperative complication rate. Secondary outcomes included length of stay, postoperative pain, and recurrence rate.
Assessment of complicationsIn our study, the intraoperative and postoperative complications were collected and reported according to the guidelines presented in the literatures [13, 14]. Chronic postherniorrhaphy groin pain is defined as pain lasting > 6 months after surgery. The statistical analysis was conducted utilizing the Clavien–Dindo classification system [15], with special attention paid to situations in which multiple complications were encountered by a single patient. Grade I complications were categorized according to the highest observed Clavien–Dindo grade within each patient.
Postoperative careTEP is usually performed under general anesthesia, requiring postoperative monitoring for 3–5 h. Postoperative management included sandbag compression on the groin area for eight hours and analgesics tailored to renal function as needed: paracetamol for those with compromised renal capabilities and ibuprofen or paracetamol for other patients. Patients were encouraged to adhere to a diet characterized by low-fat and high-protein content to support their recovery. More strenuous activity, such as running or contact sports, should be avoided for three months. Follow-up data were collected through telephone questionnaires that covered various aspects such as incision sites, pain management strategies, dietary habits, and bowel function. The Visual Analogue Scale (VAS) was utilized to evaluate the participants’ chronic pain levels. Recurrence was identified by the presence of a bulge in the inguinal region. Instances where completed questionnaires were not received from patients or repeated contact attempts proved unsuccessful, they were classified as non-respondents. The completion rates for the TD group and the PD group were 94.8% (296 out of 312) and 94.2% (147 out of 156), respectively.
Statistical analysisThe data were analyzed using SPSS 28 software. Propensity score matching (PMS) was performed on the baseline data of patients at a ratio of 1:2, with the caliper value set to 0.1. Descriptive statistics were used to analyze baseline characteristics, while T-tests or Chi-square tests were employed to compare primary and secondary outcomes between the two groups. Measurement data were expressed as mean ± standard deviation (x ± s), and comparisons between groups were made using T-tests. Categorical data were presented as cases (%). The χ2 test was used for comparisons among groups, and P < 0.05 indicated a statistically significant difference.
Comments (0)