The adult cerebral arterial circle is established through the anastomosis of the terminal branches of the internal carotid artery (ICA) along with the vertebrobasilar system, which includes the anterior, middle, and posterior cerebral artery (ACA, MCA, and PCA) [7].
However, these vessels are shaped by other embryonic arteries that undergo regression or fusion throughout embryological development to establish the adult mature arterial system. The embryonic ICA gives rise to rostral and caudal divisions that supply the brain. The rostral division is identified as the primitive olfactory artery, which supplies the prosencephalon and terminates in the nasal fossa [5]. In rare instances, this artery may persist in adulthood, resulting in the formation of the persistent primitive olfactory artery (PPOA), which has been reported to have a prevalence of 0.14%, according to a large retrospective study [11].
Contemporary literature infrequently documents the coexistence of rare variants of the cerebral arterial circle. This report delineates a distinctive arterial anatomy characterized by the amalgamation of various variants.
Anatomic variation
During an angiographic study utilizing a computed tomography angiography (CTA) archived dataset, the anatomical characteristics of a 65-year-old male patient were meticulously examined. This dataset was procured from the General Hospital of Nikaia-Piraeus after obtaining ethical approval from the relevant authorities (protocol number: 56485, date of approval: 13 November 2024). The scans were documented using Horos software version 3.3.6 (Horos Project). In alignment with findings from prior studies [8], evidence was obtained through the multiplanar reconstruction of axial, coronal, and sagittal slices alongside three-dimensional volume reconstruction.
The bilateral ICAs typically branch into the left and right ACAs and MCAs within the anterior circulation.
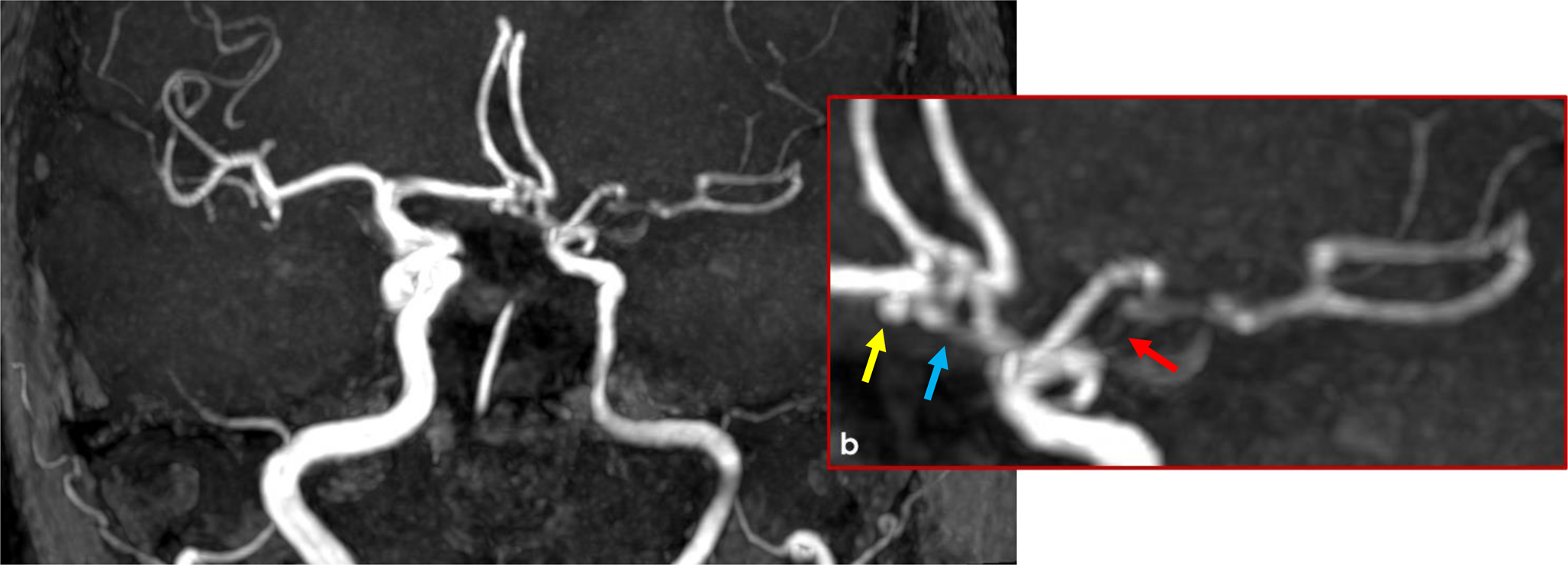
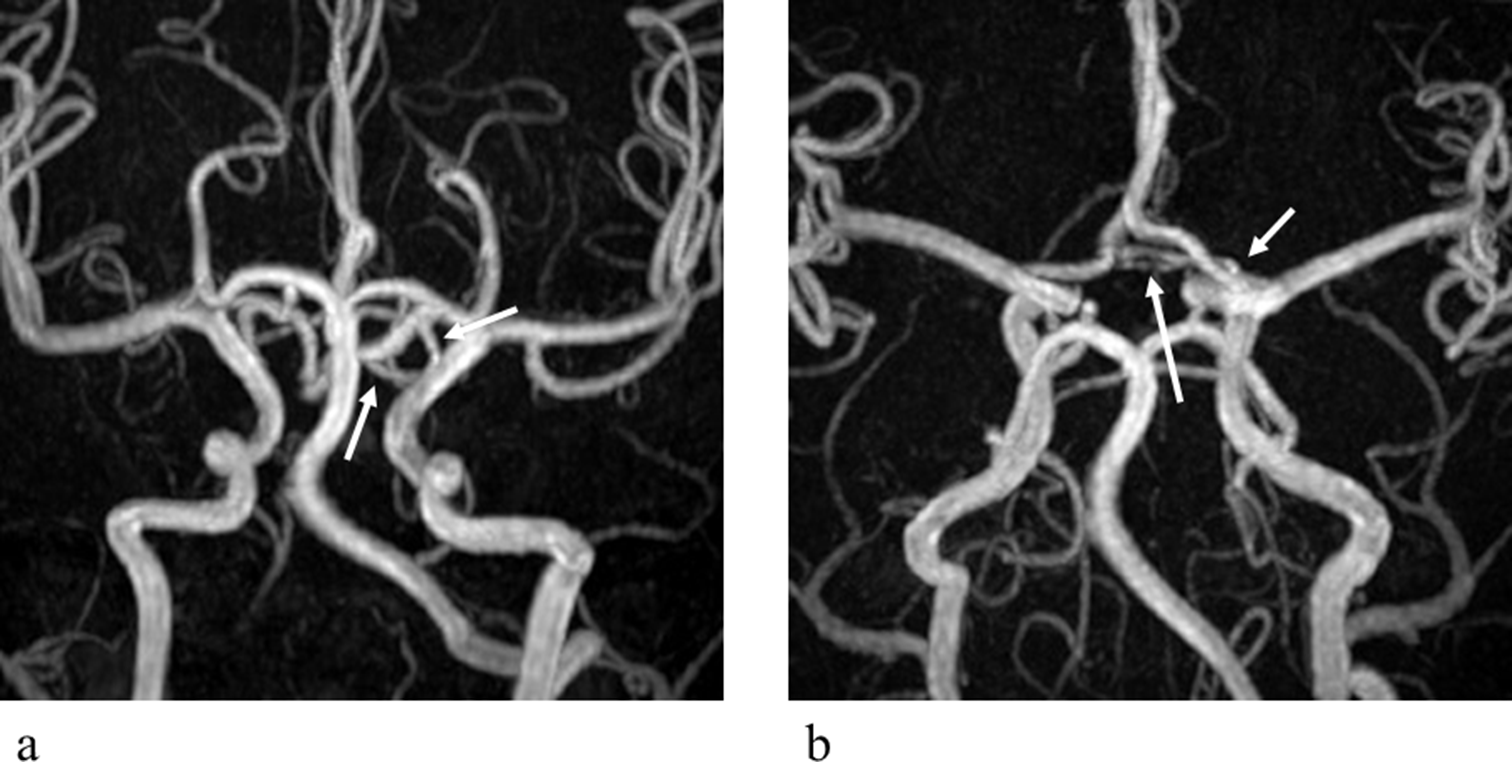
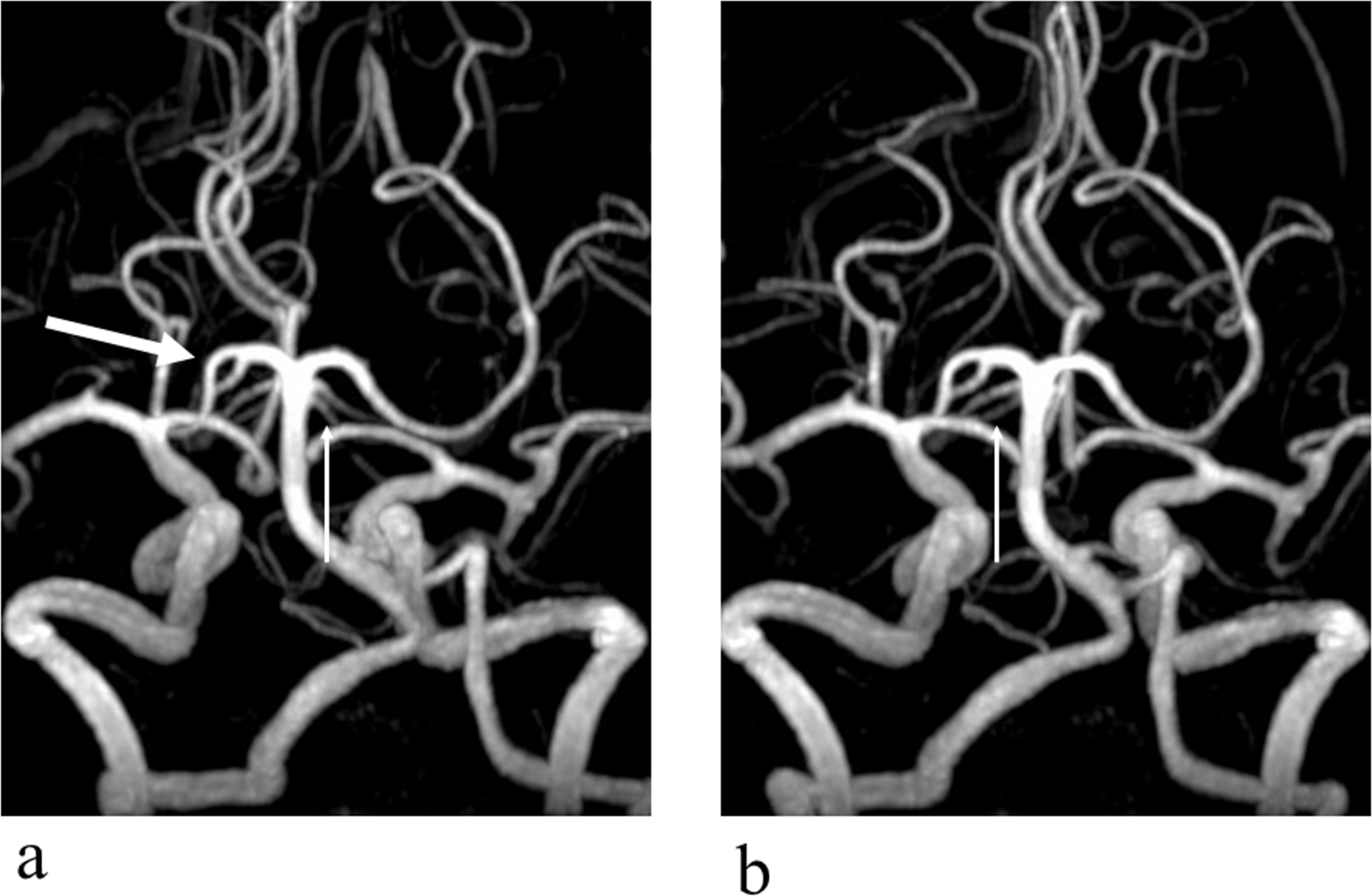
On the left side, the A1 segment measured 14.2 mm in length and 1.83 mm in diameter. At the junction of the A1 and A2 segments (A1-A2), an accessory branch (diameter of 1.2 mm) was identified, originating from this point and following a course along the left MCA; consequently, this branch was recognized as an accessory left MCA (AMCA) originating from the ACA.
The A2 segment, measuring 2.6 mm long, bifurcated into a primary branch with a diameter of 1.6 mm and followed the conventional trajectory of the contralateral (right-sided) A2 segment. In contrast, the second branch (with a diameter of 1.8 mm) pursued an anteroinferior trajectory towards the cribriform plate of the ethmoid bone, gave rise to a nasal branch, executed a hairpin turn, and continued in parallel orientation with the two A2 segments. Therefore, this branch is classified as a PPOA variant (Fig. 1).
The posterior circulation of the patient was free of variants.


Comments (0)