In this nationwide, population-based cohort of COVID-19 patients, we found an increased risk of severe COVID-19 (hospitalization, ICU treatment or death) in individuals with chronic HBV infection, even after adjusting for potential confounders. In addition to an increased risk in individuals who were male, elderly, non-vaccinated, and with low- socioeconomic status (SES), the multivariable models also showed that individuals diagnosed with HBV and born in Africa had a higher risk of severe COVID-19, including an increased risk of death due to COVID-19, compared to individuals with HBV infection born in other regions.
A potential mechanism, that could explain that persons with chronic hepatitis B with- or without cirrhosis have higher risk for severe COVID-19, is T-cell exhaustion. Chronic HBV leads to persistent antigen exposure, causing exhaustion of virus-specific CD8+ T cells. T-cell exhaustion is characterised by poor effector function, diminished proliferation, and differentiation, decreased cytokine responses, and high expression of inhibitory receptors which results in reduced capacity to control not only HBV but also other viral infections [25]. Chronic HBV infection also affects NK cells and dendritic cells, and the impact of chronic HBV infection on the immune system would therefore result in diminished immune function, with increased risk for severe disease [26, 27]. In addition, HBV patients with advanced cirrhosis, and decompensation have impaired immune regulation, placing these individuals at further risk for severe COVID-19 [28, 29]. SARS-CoV-2 infection itself contributes to liver injury, and the etiological mechanisms include severe inflammatory response, anoxia, drug-induced liver injury, direct cytotoxicity, as well as reactivation of pre-existing liver disease [30, 31]. All together, the findings in our study could be caused by the described mechanisms.
A potential explanation of our finding that individuals born in other regions than northern Europe, and especially those born in African countries, had higher risk for severe COVID-19 could be that individuals that moved to Sweden more recently lack register information on history of e.g. hospital admissions. Hence, wCCI may not fully capture and adjust for comorbidity in this group, and their higher risk may in part be caused by residual confounding. However, according to a report from the Public Health Agency of Sweden, individuals born in other countries, particularly in Africa and the Middle East, exhibited a greater risk of ICU admissions and higher mortality rates compared to those born in Sweden during the period spanning 2020-2021[32]. Similar patterns have been discerned in other Western nations(33, 34). This indicates that individuals that have migrated to Sweden, especially from African regions, might be more vulnerable to severe COVID-19.
Our study has several strengths. Our study includes all known laboratory-verified COVID-19 cases in Sweden, and thereby the proportion of included known cases is complete. Our study has a larger sample size compared to prior investigations which enhances the statistical power and reliability of our findings(18, 20, 35). By leveraging the comprehensive, nationwide data of the Swedish healthcare registers, our study cohort incorporated over 1,000,000 individuals in total, representative of the entire COVID-19 spectrum. This expanded dataset facilitated the inclusion of a diverse array of variables in our analytical model, permitting a more meticulous adjustment for potential confounding factors than was feasible in earlier studies. We also included all COVID-19 patients diagnosed with HBV on a nationwide scale. Many other studies focused mainly on hospitalized patients from a single hospital or region[36], or included patients with many different causes of liver disease[13, 37]. This study also serves to augment prior research primarily conducted in Asia, thereby enhancing the global perspective.
During the first years of the pandemic, Sweden experienced high numbers of COVID-19 cases and higher mortality compared to neighbouring countries(38). Sweden implemented widespread testing measures, and all cases confirmed through polymerase chain reaction (PCR) were reported to a national communicable surveillance database SmiNet administered by the Public Health Agency of Sweden from 1 February 2020. Sweden also has unique register data for HBV patients, with advanced screening program, and most HBV-patients are followed by the Infectious disease clinics over time. This context offers a unique opportunity to study the impact on COVID-19 and HBV on a population level. Consequently, our study offers a clinically relevant assessment of the odds ratios pertaining to the development of clinically significant COVID-19 outcomes, on a national scale.
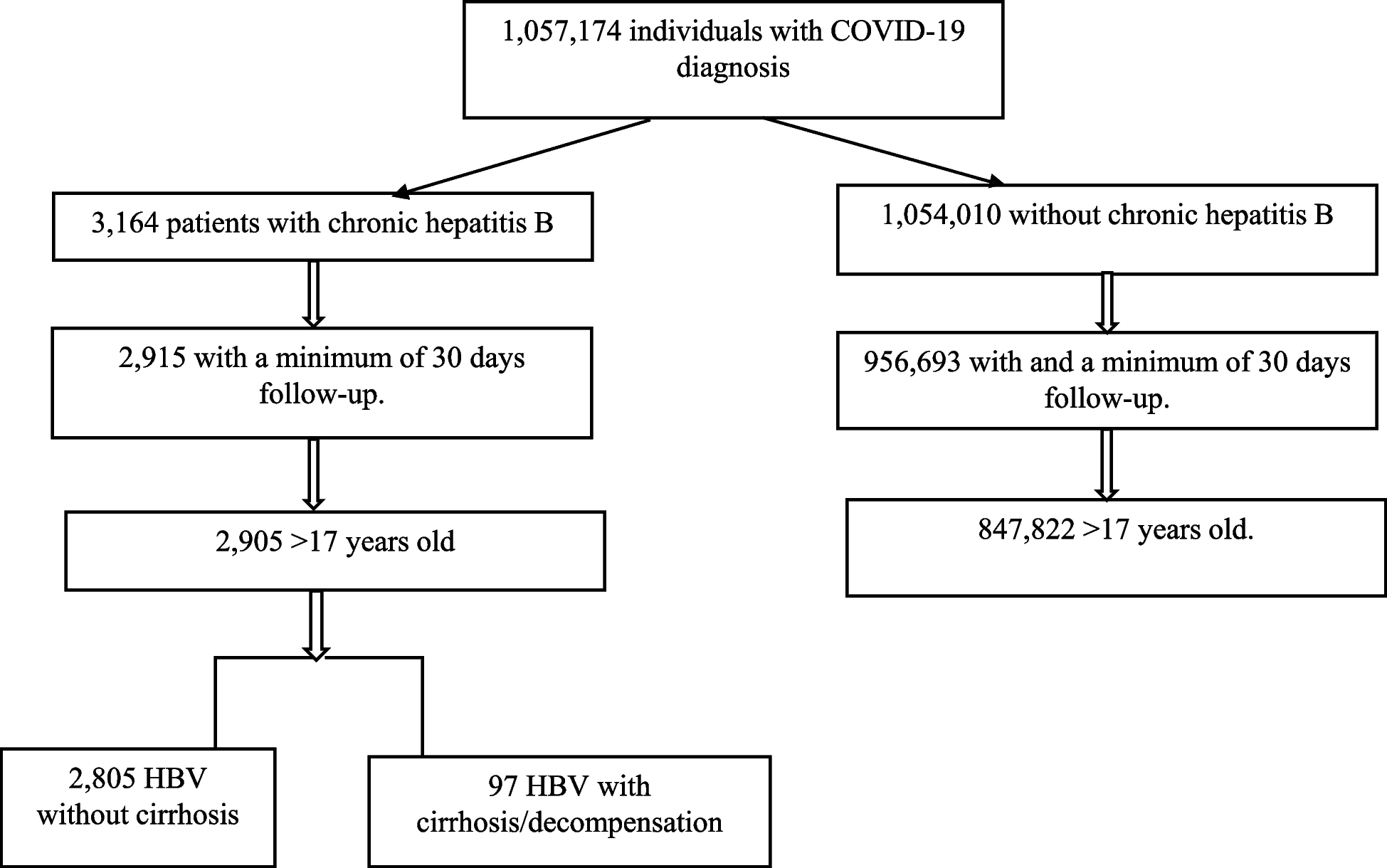
We acknowledge several limitations to our study. First, our research was conducted during the early phase of the pandemic when the alpha and beta variants of SARS-CoV-2 predominated in Sweden, and vaccination coverage was low[39]. In this period only elderly, or people with severe co-morbidities, were prioritized for vaccination, which is reflected in our univariable analysis where initially COVID-19 vaccination associated with severe COVID-19. However, following adjustment, the COVID-19 vaccine protected against severe COVID-19. Given the emergence of new variants and increased vaccination rates, the applicability of our findings to the current context may be limited. Second, identification of patients with cirrhosis/decompensation relied on diagnosis codes. This method identified only 98 individuals in the HBV with cirrhosis/decompensation group, and there is a possibility that some individuals meeting these criteria may not have received a formal diagnosis from their physicians. We also acknowledge the risk of missclassification, for example if patients with HBV infection have not been registered with a HBV diagnosis in any of the Swedish registers used in this study, which may affect the results. However, considering the strong associations in the results, the risk of underdiagnosed HBV infection is unlikely to have a major affect on the outcomes. Third, due to the utilization of national registers in our study, we lacked serological, laboratory and clinical data regarding liver function and HBV status, which could be of importance when interpreting the results.
In addition to the primary outcome, we analyzed several secondary outcomes, and outcomes stratified by cirrhosis and HBV. The reported p-values and confidence intervals were not adjusted for multiple testing. However, the results from the different analyses were in overall agreement.






Comments (0)