2.1 Sex as a Biological Variable
This study focuses on individuals of female sex. As a women-specific initiative, male individuals did not participate in the campaign.
2.2 Study Type and Aim
Following the World Heart Day 2023, a women-specific cardiovascular prevention pilot campaign (“Cuore di Donna in Farmacia”, i.e. “Woman's heart in pharmacy”) endorsed by the non-profit organization Cittadinanzattiva [6], in collaboration with the Italian Reference Centre for gender medicine [8], Fondazione Onda [9], the Italian Society of Hypertension (SIIA) [10], and the Italian Society of Cardiovascular Prevention (SIPREC) [11], was conducted from October 16th to November 10th, 2023 in Italian pharmacies of the National Federation of Pharmacies (Federfarma [7]) network enabled for telemedicine services in the provinces of Brescia (Lombardy, Northern Italy), Ancona, Ascoli Piceno, Fermo, Macerata, Pesaro-Urbino (Marche, Central Italy), and Palermo (Sicily, Southern Italy). The initiative aimed at evaluating the effectiveness of screening activities offered by pharmacies and raising awareness of cardiovascular health status among Italian women through the assessment of their risk profile and the identification of their major health concerns.
2.3 Population
Volunteer women aged 40 and over entering the participating pharmacies during the campaign period were enrolled.
2.4 Outcomes
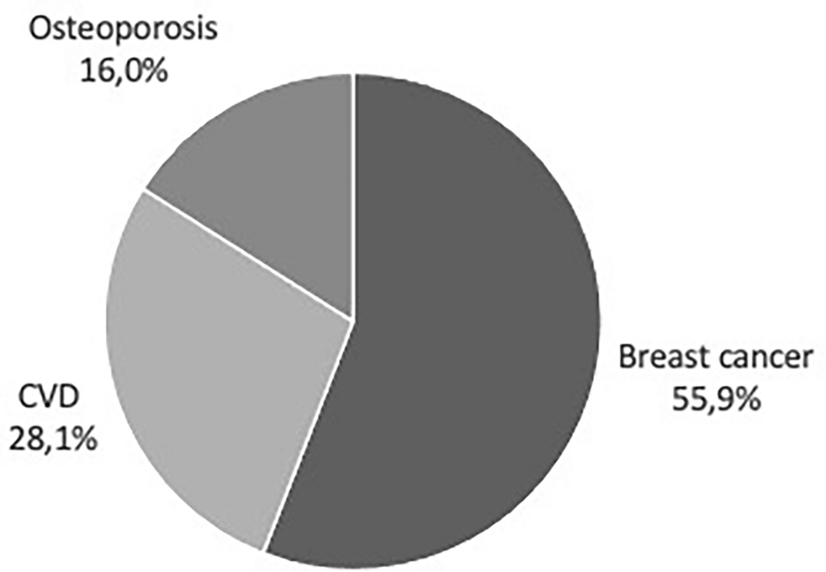
The primary outcome of the present study was the prevalence of cardiovascular risk factors and diseases among participating women. Secondary outcomes included the awareness of CVD burden relative to other common female-specific diseases (breast cancer, osteoporosis), the prevalence of electrocardiographic abnormalities, and the estimated cardiovascular risk in the examined population.
2.5 Compliance with Ethical Standards
The survey was conducted in conformity with the Helsinki Declaration [12] and the European General Data Protection Regulation (EU GDPR), article 89 [13].
2.6 Ethical Approval
As an observational study, where de-identified data were collected, ethical approval was deemed exempt. The collection of de-identified data at enrollment prevents any possibility to identify study participants.
2.7 Study Procedures and Related Variables
Participants answered an anonymous questionnaire on their demographic and clinical characteristics and lifestyle habits (age, whether on menopause, early menopause < 45 years, hormonal replacement therapy within 10 years after menopause, diagnosed/treated hypertension, smoking habits, family history of early CVD, diabetes, diagnosed/treated hypercholesterolemia, diagnosed atrial fibrillation [AFib], HF, chronic kidney disease [CKD], any established CVD and/or CKD, at least 30’/day of physical activity, everyday use of vegetables/fruits, unlimited salt use; mobile/missing/elongated teeth; spontaneous/on brushing gingival bleeding [14], diagnosed periodontitis [15]) and underwent measurement of essential anthropometric and clinical parameters (weight in kilograms [kg], height in meters [m], waist circumference, seated systolic and diastolic blood pressure [BP], seated heart rate [HR], 12-lead electrocardiogram [ECG]). All data were collected or measured by trained pharmacists. Established CVD/CKD included personal history of valvular heart disease, angina, heart attack, HF, stroke, transient ischemic attack (TIA), atherosclerotic disease, peripheral arterial disease, aneurysm, AFib, and CKD. Body mass index (BMI) was calculated as weight (kg) divided by height in meters (m) squared, and participants were classified accordingly as being underweight (BMI<18.5 kg/m2), normal weight (BMI 18.5 to 24.9 kg/m2), overweight (BMI 25 to 29.9 kg/m2), or obese (BMI ≥30 kg/m2). BP and HR were measured using validated, semi-automated sphygmomanometers according to standard procedures [16], and the average of the 2nd and 3rd readings was calculated and recorded. 12-lead ECG was recorded with dedicated devices centrally connected in telematic mode with Health Telematic Network (HTN)-Virtual Hospital [17], thereby allowing real-time telereporting by the cardiologist on duty [18]. ECG variables of interest included the presence of abnormalities in heart rhythm, atrio-ventricular and intraventricular conduction, Q-wave, ST trait, ventricular repolarization, and the presence of ectopic heart beats. In case of abnormalities, further diagnostic investigations (dynamic ECG; echocardiogram) and/or clinical assessment (referral to the treating doctor; referral to cardiologist consultation; referral to the nearest hospital for emergency assessment) were indicated in real time by the cardiologist, as appropriate.
2.8 Statistics
Demographic and clinical data entered on the online questionnaire and ECG variables of interest were centralized at the Federfarma coordinating center, where they were transferred to an electronic spreadsheet for analyses.
Unpaired Student’s t test and chi-squared test were used to detect differences in quantitative (mean ± standard deviation [SD]) and qualitative (N, %) data, respectively (statistical significance: p < 0.05). BP was used as a continuous (mmHg) and categorical variable. BP<130/85 mmHg was considered normal BP; BP 130–139 and/or 85–89 mmHg was considered as high-normal; BP ≥140 and/or 90 mmHg was considered as hypertension (grade 1: 140–159 mmHg systolic BP and/or 90–99 mmHg diastolic BP; grade 2: 160–179 mmHg systolic BP and/or 100–109 mmHg diastolic BP; grade 3: ≥180 mmHg systolic BP and/or ≥110 mmHg diastolic BP) [16]. BP profile and hypertension prevalence and classification (normal BP, high-normal BP, newly diagnosed hypertension; controlled/uncontrolled hypertension) overall were assessed based on BP measurements, age, and hypertension history and treatment [19]. The prevalence of comorbidities was assessed overall and among participants with ECG abnormalities.
A simplified algorithm for the estimation of cardiovascular risk according to BP grading, modified from [16], was applied, based on the BP profile and the associated cardiovascular risk factors. Cardiovascular risk was then defined as absent, low, low-moderate, moderate, moderate-high, high, and very high [16] (Supplementary Table 1).
Multiple response analysis was performed to assess the frequency of different combinations of variables (early menopause, hormone replacement therapy within 10 years after menopause, physical inactivity, unhealthy diet habits including poor consumption of vegetables/fruits, self-reported signs of gingivitis/periodontitis, diagnosed periodontitis) in women across different categories of estimated cardiovascular risk (“low”, if low to no risk; “moderate”, if low-moderate, moderate, or moderate-high risk; “high”, if high to very high risk). The relative UpSet plot, showing intersections in a matrix whose rows correspond to given factors and the columns to the intersections between the same factors, was generated with the dedicated R package (v 4.2.1).
Data were analyzed as recorded, without imputation for missing data.


Comments (0)