Limitations of the Study
There are two main limitations in diagnosing diseases in skeletal remains from archaeological sites: Taphonomic processes can alter bone and destroy formerly present pathological changes or they might simulate characteristics of diseases. In the presented case, postmortem destruction of the lesion´s walls is visible, however, this does not hinder the diagnosis based on other distinct features: Replacement of compact by woven bone and the presence of cementum-like materials are particularly clearly visible in the microscopic analysis. The second limitation is the missing soft tissue, laboratory values, and the patient´s clinical history. Without this information, diagnosing is challenging, but not impossible.
Differential Diagnosis and Probable Diagnosis
Applying differential diagnosing, we were able to narrow down the diagnosis, even in a 4500-year-old skeleton: The combination of woven bone and cementum-like materials in microscopic evaluation could encompass odontogenic fibroma, cementoblastoma, ossifying fibroma, and cemento-osseous dysplasia [1].
The odontogenic fibroma is a very rare neoplasm, mainly located in the region of the mandibular premolars [18]. It comprises soft tissue components (odontogenic epithelium and fibrous stroma) rather than mineralized materials like woven bone or cementum [18]. If dysplastic cementum or osteoid is present, it is only focal within the lesion and does not show a conglomerate [18].
A cementoblastoma is unlikely as there is no evidence of blending with the root of a tooth or root resorption [19]; instead, the cementum-like tissue is separate from the roots of the teeth. Furthermore, the preferred location of the permanent first mandibular molar does not match the localization of the resorption in the presented case [19].
Ossifying fibroma (OF) cannot be excluded by its composition of mineralized materials of varying appearances [20]. However, its preferred location in the posterior mandible [21], its often-occurring jaw expansion, and larger size lesions [22] do not match the features of the presented case. While radiographically the presence of a well-defined border rather points to OF than cemento-osseous dysplasia (COD), the mixed radio-opacity is characteristic of COD [22]. Furthermore, OF cases are less often related to tooth apices than COD [22].
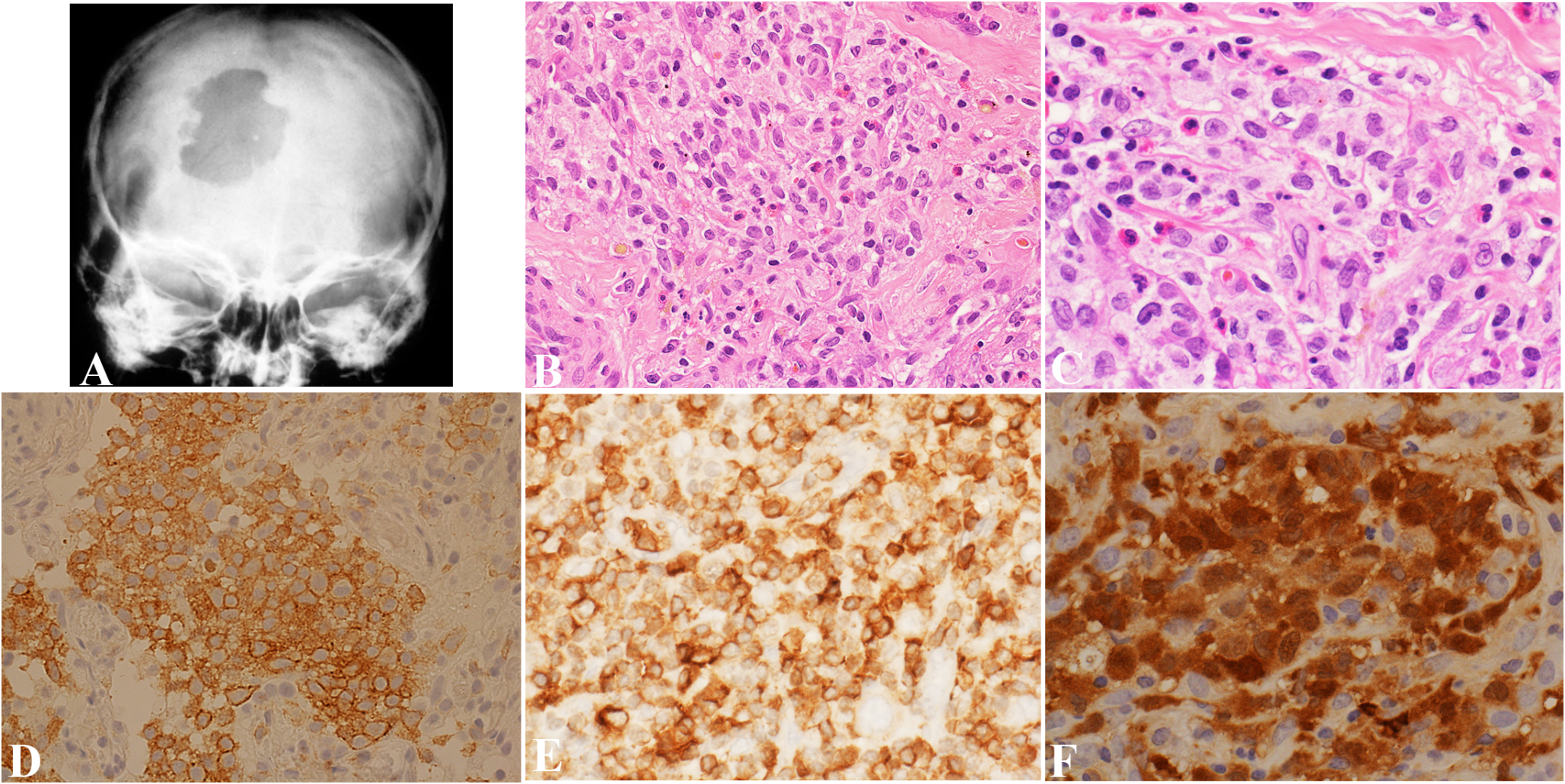
Cemento-osseous dysplasia is the most frequently occurring fibro-osseous lesion of the jaws [23] and is located in the periapical region of the tooth-bearing areas, predominantly of the mandible [24, 25]. Its main characteristic feature is the replacement of normal bone by metaplastic bone mixed with fibrous tissue [24] in close association with tooth apices. Radiology and computed tomography images of this case show a mixed lesion with a well-defined radiolucent rim around the radiopacity, characteristic of an intermediate stage [22]. The large lesion which shows a fusion of periapical lesions of alveoli 32 and 31 shows more mineralization than the exclusively radiolucent lesions of alveoli 41 and 42.
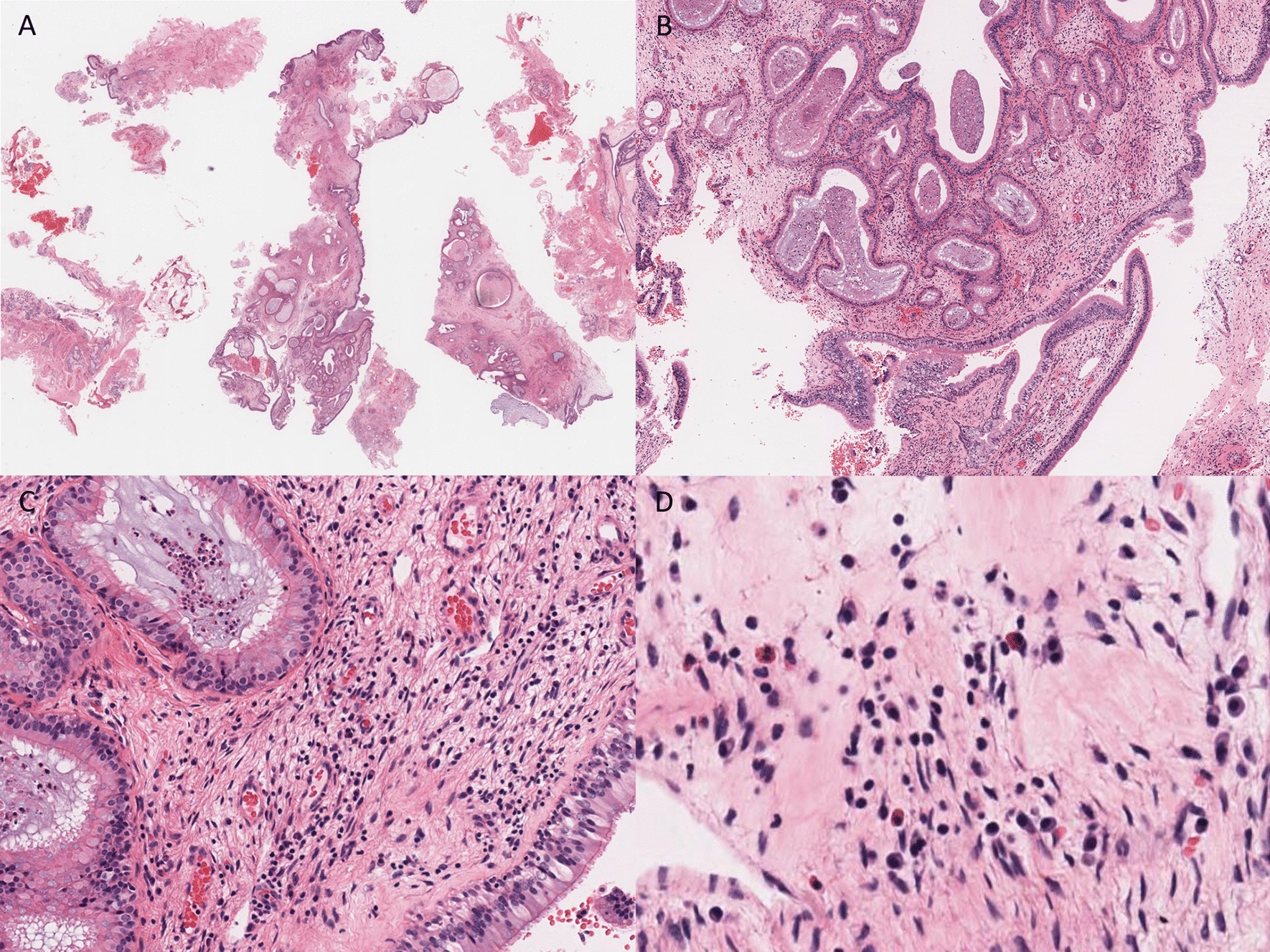
Apart from the missing cellular fibrous tissue caused by taphonomic reasons, microscopically, woven bone and cementum-like material are detectable. One important aspect in favor of the diagnosis of COD is the missing fusion of the hard tissue components with the roots of the teeth. The latest edition of the WHO classification [26] lists four different subtypes of COD: the best fitting is the periapical COD which has multiple foci in the region of the lower incisors.
Contextualizing of the Oldest Case of COD from the Bronze Age
The presented case of COD in a 30-40-year-old female individual from the Bronze Age burial mound cemetery of Budyonnovsk in the Northern region of the Caucasus is the oldest evidence of such a disease in humans so far. Within this cemetery, buried in close vicinity, a 22-25-year-old male individual (burial 14) showed a similar pathology, a unifocal cemento-osseous dysplasia of the alveolus 43 [6]. Both individuals share similar grave goods and types of grave construction indicating that they might have been buried during the same period, the Late Catacomb, more precisely, the East Manych Catacomb Culture, which dates to 2500 − 2300 BC. Archaeologically, burial 2 is earlier than burial 14, but the chronological gap is small, and as such both individuals could have lived contemporarily or individual 14 was born later than individual 2. The probability that two individuals sharing the diagnosis of cemento-osseous dysplasia and who are buried in one burial mound might be biologically related, is worth being discussed. Although a familial basis of florid cemento-osseous dysplasia is known [27], familial cases of periapical are less often reported [28]. Genetic analysis is planned to detect a possible biological relationship between the two affected individuals and depending on the bone preservation to search for hotspot mutations involving the RAS-MAPK signaling pathway, which were identified to be responsible for 28% of COD cases [5].
The benefit of samples from archaeological skeletons is the availability of bone tissue which is neither decalcified nor scarce because it has not to be taken from a living person. Therefore, we hope to get enough tissue samples to perform a sufficient genetic analysis. Furthermore, unconventional views on the lesions are possible using samples of paleopathological research: They can provide a macroscopic view of the lesion and surface details, which is impossible in a living patient.
The oldest two cases of COD from the Bronze Age show that this disease has a long, yet unknown, history of occurrence and did not seem to have changed in its appearance over the last 4500 years.






Comments (0)