TL is the most common form of leishmaniasis, with over 1 million new cases each year worldwide [17]. If not properly treated, the disease can leave life-long scars and cause serious disability or stigma.
Although not fatal, TL has a socioeconomic impact due to the stigmatization of individuals who may present disfiguring lesions when infected and even after being cured. Leishmania braziliensis is responsible for ML in Latin America [2]. A small percentage of persons infected with L. braziliensis develop mucous membrane involvement of the nose, oral cavity, pharynx, or larynx months to years after their skin lesions have healed [2–3]. Mucosal disease can occur because of infection due to other parasite species, including L. tropica (18–19), L. donovani [20–21–22–23–24] and L. infantum [3–[25-[26−[12-[16. L.infantum-associated ML appears to be more frequent than previously expected and manifests as localized mucosal disease in the absence of concomitant visceral or cutaneous leishmaniasis.
Tonsillar leishmaniasis can be detected in cases of multiple mucosal and/or visceral localization, nonetheless this series includes 5 cases of TL with exclusive localization in the tonsils. The exact mechanism of isolated mucosal/oropharyngeal disease without skin involvement remains unclear. Mucosal leishmaniasis is thought to arise not from a direct bite at the mucosal site, but rather as a metastatic consequence of an earlier, unnoticed cutaneous infection that subsequently spread to mucosal tissues [3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27].
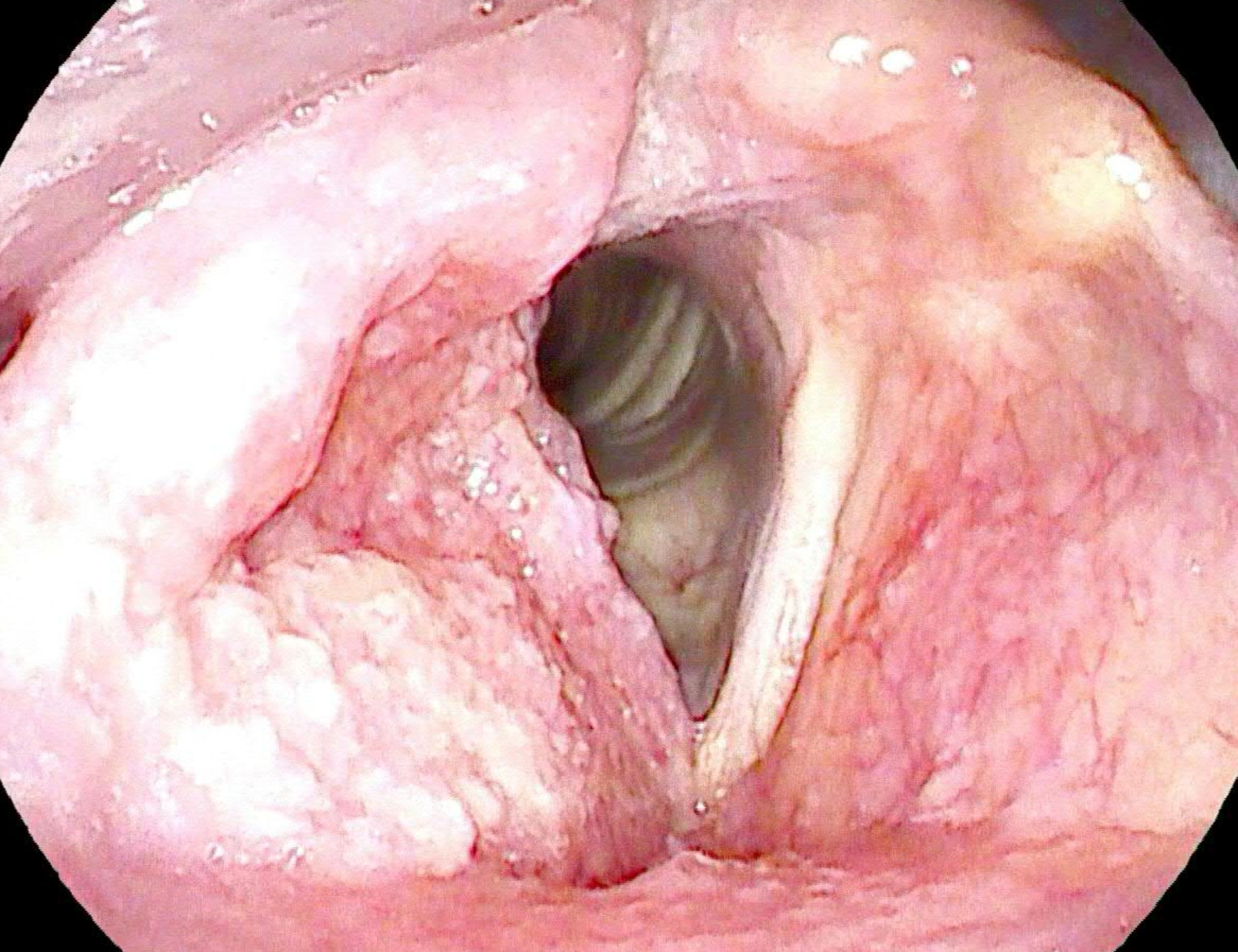
The broad spectrum of ML clinical symptoms can complicate the process of obtaining an accurate diagnosis. Indeed, clinical manifestations of ML are variable and often nonspecific, including nodules, polypoid lesions or granular inflammation and may involve the buccal area, pharyngeal and laryngeal regions and, less frequently, the nose [28]. ML is often misdiagnosed with other upper respiratory tract diseases, particularly cancer, since they frequently present with ulcerated and bleeding masses. Due to the overlap in the clinical presentation of ML and neoplasia, leishmaniasis should be taken into consideration in the differential diagnosis of head and neck cancer, especially in patients from endemic areas or who report travelling to endemic countries [29].
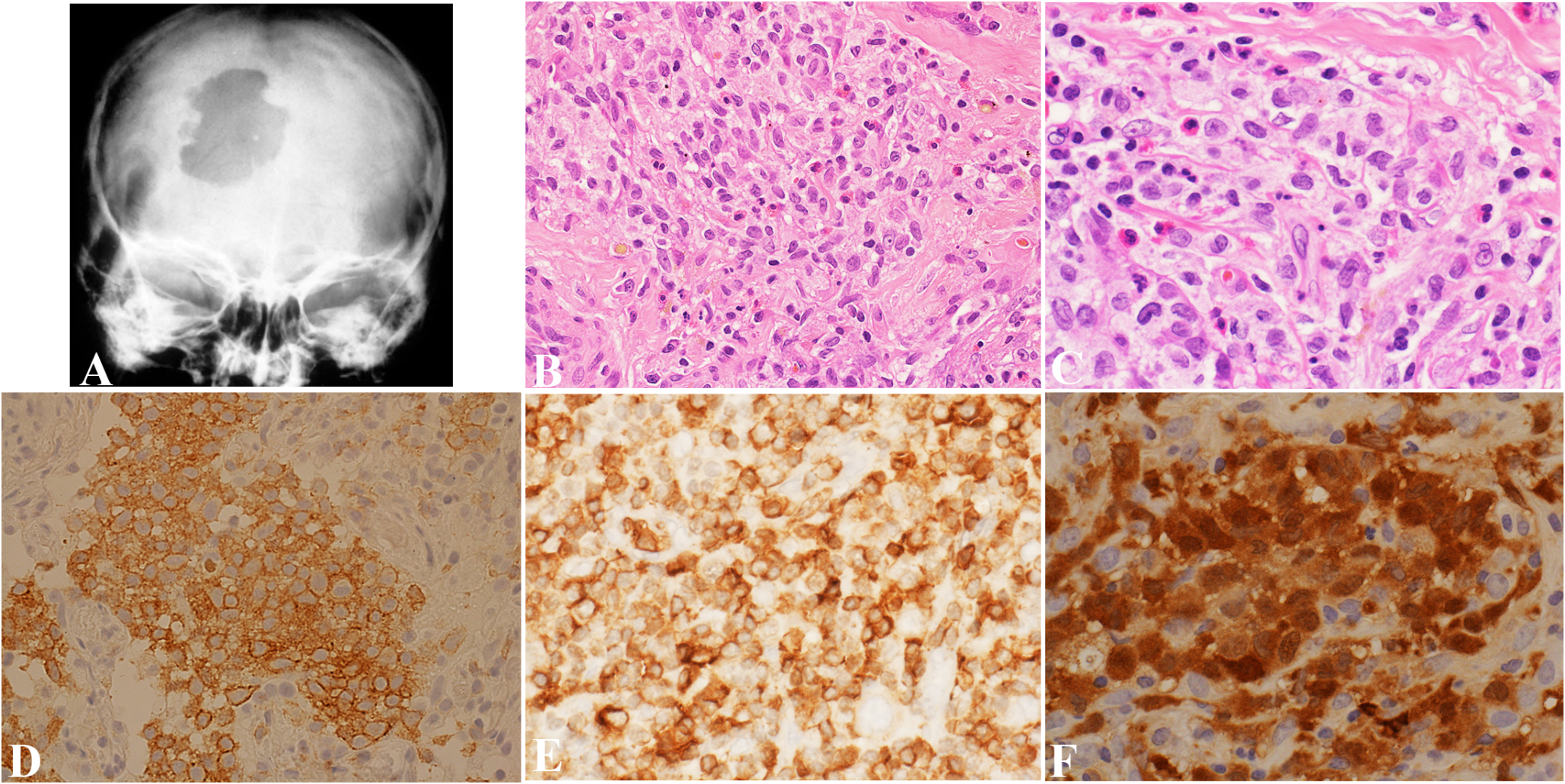
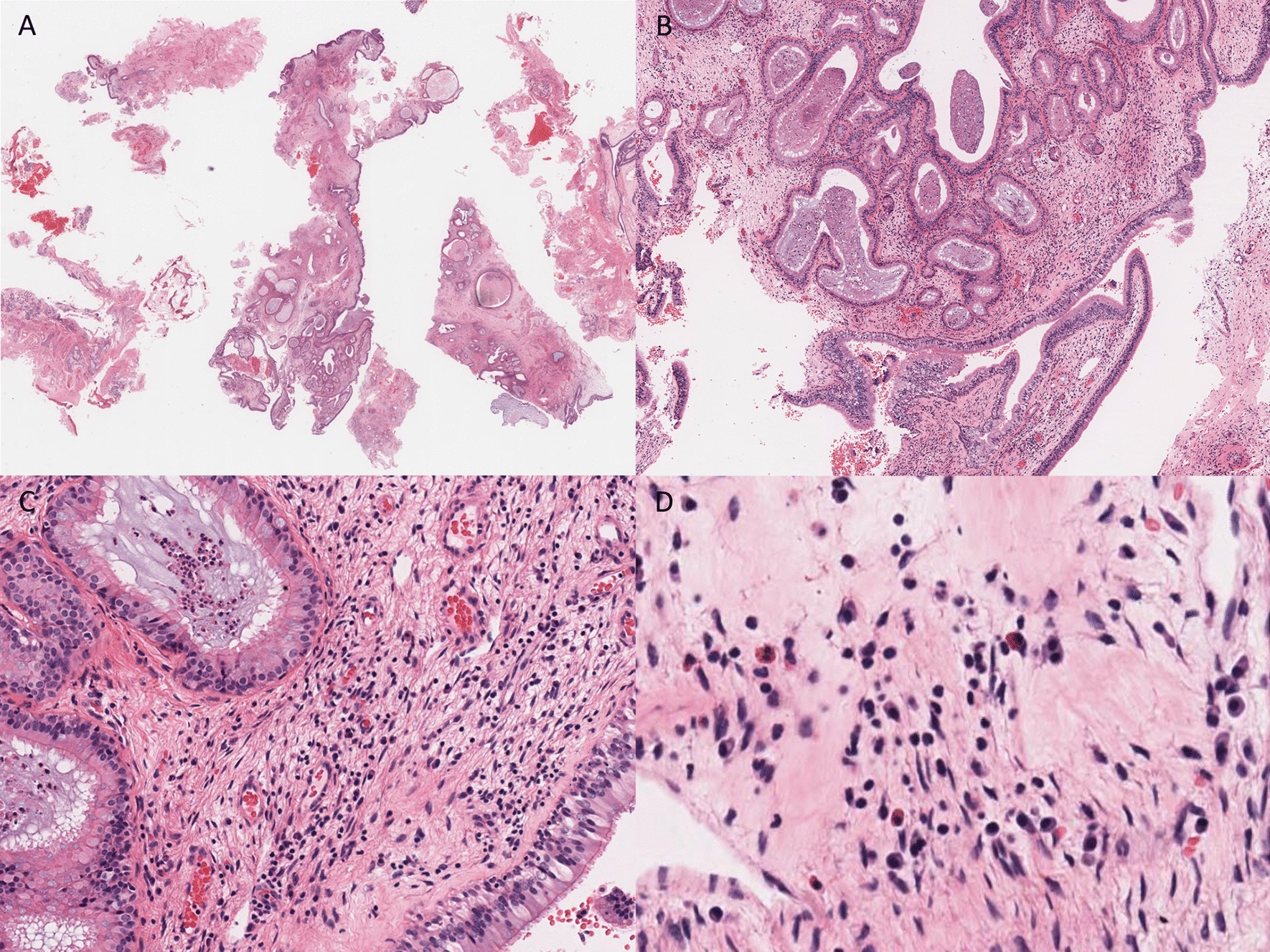
On histology all cases presented multiple non-necrotizing granulomas. Tonsillar granulomatous lesions can have multiple aetiologies, among which infectious and non-infectious conditions should be considered. In the present cases, tuberculosis and sarcoidosis were excluded by clinical, radiological and laboratory tests. In 4 out of 5 cases amastigotes were detected either on H&E only or with the CD1a immunostaining, while in 1 case TL was suspected considering the recent increase of TL cases in northeastern Italy [1].
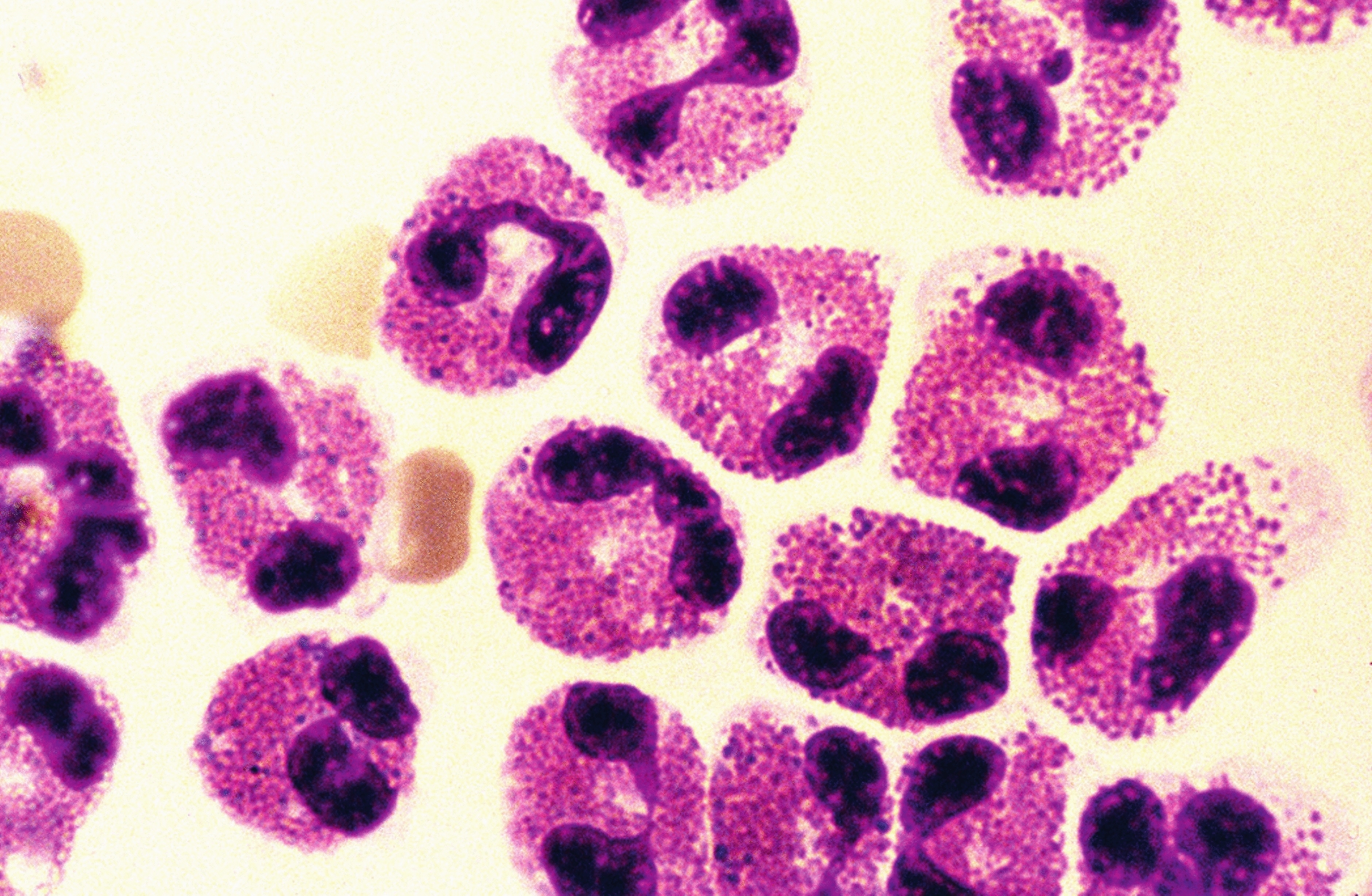
Other differential diagnoses to consider for parasitized histiocytes in the oropharynx, besides tuberculosis, include histoplasmosis, cryptococcosis, and talaromycosis. All these infectious diseases are caused by pathogens that can trigger a granulomatous immune response, which varies from being absent in immunocompromised individuals to forming large necrotizing lesions in people with an immunocompetent immune system. The diagnosis of TL is based on the precise identification of the causative pathogen [17]. For this purpose, conventional methods such as microscopic examination of samples stained with hematoxylin-eosin (H&E), Giemsa, Grocott and periodic acid–Schiff (PAS), specific cultures, and PCR amplification of Leishmania DNA are used. Amastigotes appear as round to oval basophilic intracytoplasmic inclusions, approximately 4 μm in size, found in varying numbers within the cytoplasm of histiocytes [30]. They contain a single, dense, eccentric nucleus and a rod-shaped kinetoplast, which can be oriented either perpendicular or parallel to the nucleus. Kinetoplasts can be challenging to observe in fixed sections of Leishmania-infected tissue, regardless of the staining technique used. This difficulty is especially pronounced in sections stained with hematoxylin and eosin. Other pathogens that must be microscopically differentiated include: Histoplasma capsulatum, Cryptococcus neoformans and Talaromyces marneffei [31]. These pathogens are approximately the same size and primarily found within macrophages and histiocytes. Moreover Histoplasma capsulatum and Cryptococcus neoformans infections may occasionally occur in Italy (32–33), complicating the interpretation of epidemiological data.
Histoplasma capsulatum causes histoplasmosis, a systemic fungal infection affecting humans and animals, often linked to HIV. Since the 1980s, it has become a significant opportunistic infection in AIDS patients. Histoplasma capsulatum appears in round or ellipsoidal forms, and the cell membrane is not distinctly visible. A purplish nucleus, occupying about one-third to one-half of the spore and the cytoplasm appeared light blue. Peripheral spores are seen as empty, bright, colorless rings, resembling a capsule, a sort of halo-like ring around the cell, and display narrow-based budding, often forming clusters of numerous organisms and they are strongly positive for PAS, while amastigote forms of Leishmania spp are not stained. The distinctive kinetoplasts of Leishmania, which generally stain more intensely than the nucleus, are not present in Histoplasma capsulatum.
Cryptococcus is a yeast with a protective capsule, commonly found in the environment. It is a globally distributed opportunistic fungal pathogen, and it has been isolated from sources such as pigeon droppings, decomposing wood, fruits, and vegetables. Individuals with weakened cell-mediated immunity, including those with HIV, organ transplant recipients, and patients on long-term corticosteroid therapy, are at the highest risk of developing cryptococcal infections. Cryptococcus neoformans is typically identified in tissue sections as a round yeast, both intracellular and extracellular, ranging from 5 to 10 μm in size with some variation. It possesses a thick polysaccharide capsule, which creates a clear halo-like space in H-E staining and shows positivity with Alcian blue staining. Although histopathological criteria can often help distinguish cryptococcosis from histoplasmosis, differentiating between these infections can sometimes be challenging, and their treatments differ. However, the presence of yeasts with indentations or irregular depressions in their cell walls may be more indicative of cryptococcosis rather than histoplasmosis [34].
Talaromycosis is a serious fungal infection caused by Talaromyces marneffei, formerly Penicillium marneffei, a thermally dimorphic fungus and major pulmonary pathogen. It can spread through the lymphatic system or bloodstream, causing life-threatening complications. More common in warm, humid climates, it is prevalent in Southeast Asia, northern India, and southern China, affecting individuals with travel history to these regions [35]. T. marneffei pathogens are primarily found within the cytoplasm of macrophages, with a few scattered extracellularly. The yeast forms of T. marneffei appears round, ellipsoidal, or sausage-shaped, featuring one or two small purplish-red nuclei and a light blue cytoplasm. The pathogens varied in size, ranging from 2 to 8 μm, and their cell walls were not distinctly visible. In PAS staining, however, T. marneffei cell walls appeared red, well-defined, and continuous [36]. As our patients did not report travels to Asia, we did not consider it as a potential differential diagnosis.
Althoughthe distinction on the H-E-stained slide may be difficult, PAS and Grocott-stained slide could help to solve this diagnostic issue (positive stain in H. capsulatum, in Cryptococcus neoformans and in Talaromyces marneffei and negative stain in Leishmania spp.).
However, in more advanced lesions, a dense tuberculoid or sarcoid granulomatous infiltrate may be observed, along with a reduction in the parasitic load. In such cases, skin or mucosal biopsies might reveal very few or even an almost complete absence of amastigotes, making additional techniques necessary to highlight the parasite’s presence [37]. In these cases, immunohistochemistry using anti-CD1a or anti-Leishmania antibodies has shown greater sensitivity for detecting amastigotes and a valuable tool that can facilitate pathogen detection (38–39).
Additionally, the detection of Leishmania parasites DNA via PCR offers even greater sensitivity, ranging from 75.7 to 100%, while maintaining a specificity of 100%. Both histological and molecular tools demonstrate high diagnostic accuracy [40]. In our cohort of patients, in 4 out of 5 cases amastigotes were detected either on H&E only or with CD1a immunostaining, while in 1 case ML was suspected considering the recent increase in TL cases in northeastern Italy and was subsequently confirmed by PCR.
Most previous studies utilized the CD1a antibody from Novocastra/Leica Biosystems, derived from the MTB1 clone. Gadelha et al. conducted a comparison between the MTB1 and O10 clones, demonstrating that the MTB1 clone provided greater sensitivity, specificity, and accuracy [41]. In contrast, Lopez-Trujillo et al. used the routine CD1a (EP3622) Rabbit Monoclonal Antibody from Ventana-Roche Tissue Diagnostics, which showed a homogeneous staining pattern, often with greater intensity at one pole [40]. In this study (in 3 out of 5 cases), the CD1a (EP3622) Rabbit Monoclonal Antibody from Ventana-Roche Tissue Diagnostics was used. It is also important to highlight that from a histological perspective, in all analyzed cases, the squamous epithelium showed significant hyperplastic and regenerative changes, but there were no morphological features indicative of dysplasia and/or neoplasia.
According to the WHO, the treatment of ML varies between countries, considering the infecting species. Current treatments offer varied efficacy rate and diverse systemic effects that often lead to the patient abandoning treatment. In each case therapy is tailored according to clinical presentation, infecting Leishmania species and immunological status of the patient [42]. Patients must undergo to systemic treatment prevent morbidity, as disfigurement, and mortality related to aspiration pneumonia and/or respiratory obstruction [29].
The treatment strategy used in the current cases mirrored the successful therapeutic approach adopted in three previous ML cases [29]. All patients reached a complete remission after systemic treatment. At present, there is no standardized treatment for ML. In each case therapy is tailored according to clinical presentation, infecting Leishmania species and immunological status of the patient [43]. Drugs with distinct activity against Leishmania, including liposomal amphotericin B and pentamidine were used. Amphotericin B (AmB). AmB can accumulate on membrane surfaces, disrupting Leishmania cells by extracting crucial lipids, ultimately causing cell death. This interaction is significantly stronger than its binding to cholesterol in human cells, emphasizing its selective affinity, which is essential for its mechanism of action. The main limitation of AmB is its poor water solubility, which led to the use of its nephrotoxic deoxycholate formulation as a second-line therapy for VL, CL, and MCL since the 1960s. The introduction of liposomal delivery systems in the 1970s enabled the development of AmBisome, a liposomal formulation designed to enhance bioavailability and minimize toxicity [44]. Pentamidine, a synthetic amidine derivative became a treatment option for drug-resistant CL in the 1970s [45]. Pentamidine interacts with nucleic acids, interfering with nucleotide incorporation and oxidative phosphorylation, which in turn disrupts the synthesis of DNA, RNA, phospholipids, and proteins. Additionally, this drug may bind to kinetoplast DNA, inhibiting mitochondrial respiratory chain complex II and triggering apoptosis by increasing intracellular calcium levels [44].
Combined dermatological and otolaryngologist follow-up after treatment is important for the clinical management of ML. A biopsy of the lesion is mandatory to perform a parasitological diagnosis, thus allowing the prompt introduction of a correct antileishmanial therapy.






Comments (0)