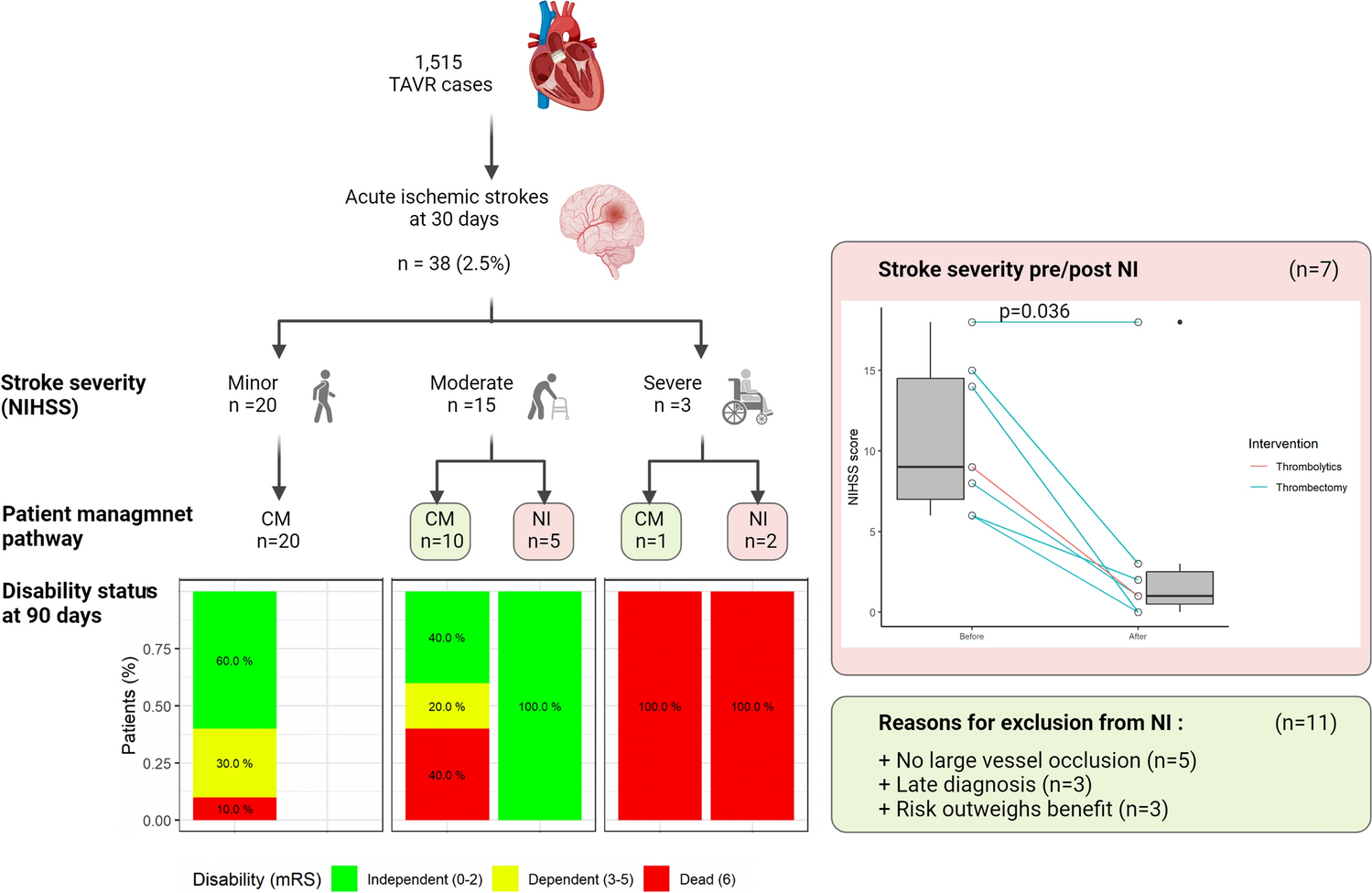
In this registry-based study, which included 1515 consecutive TAVI procedures performed between 2008 and 2021, we have identified 38 (2.5%) AISCT events within 30 days. Most AISCT occurred within the first 24 h of the procedure (57.8%). A detailed analysis of these patients revealed that approximately half had mild stroke and fewer than 10% had a severe stroke. AISCT was associated with a fourfold increase in 1-year mortality (p < 0.01). As compared to mild stroke, moderate stroke or worse was associated with a 3.7-fold increase in mortality (p = 0.038). Prior ischemic stroke, atrial fibrillation/flutter, PVD, GA, and non-femoral access emerged as risk factors for AISCT. Among 18 patients who were considered candidates for NI (moderate or severe stroke), 6 underwent attempted MT and one patient was given TT with a median NIHSS decline from 9 to 1 (p = 0.036). As compared to the CM, NI was not found to reduce mortality. However, patients with moderate severity stroke (NIHSS score 6–14) who underwent NI, enjoyed a higher rate of disability free survival at 3 months compared to patients treated conservatively (p = 0.044).
Contemporary studies have consistently demonstrated 30-day AISCT rates approximating 2–3% [9, 10]. Given that: (a) stroke is associated with a significant increase in mortality, (b) roughly 50% of AISCT could be considered moderate or severe and are potentially disabling strokes, (c) AISCT is a largely stochastic event with no available high-quality models or risk scores to predict, (d) patients consider stroke a worse outcomes than death [11], and that (e) despite the extensive experience with cerebral embolic protection devices (CEPDs) no strategy has been shown to consistently prevent AISCT [12,13,14], AISCT remains a concerning issue in the current TAVI practice.
The management of AISCT is challenging. In this regard, we have previously published data from a large multicenter cohort of 39 NI (13 TT, 26 attempted MT) in 387 AISCT events (The ASTRO-TAVI registry [15]), showing that NI may be beneficial in increasing rates of independent survival at 90 days (from 37.5 to 60% in moderate severity stroke, p = 0.016). We have thus advocated for the formation of institutional rapid response heart-brain teams to enable a timely response to AISCT and to facilitate NI when appropriate in a timely manner. Interestingly, in the ASTRO-TAVI, only approximately 25% of the patients with moderate or severe stroke underwent NI, of which 33% were given TT, potentially putting patients in an increased hazard of bleeding and vascular complications given recent large bore vascular access, in addition to an increased risk of cerebral hemorrhages given the typical characteristics of TAVI patients in combination with frequent blood pressure fluctuations. This was largely affected by a lack of interventional neuroangiograhpy capabilities in some of the participating centers.
To further explore dilemmas and strategies in ASICT management, in the current analysis we have studied our singular institutional experience of AISCT in a higher granularity. Rabin medical center is a tertiary hospital with an onsite neurology consultant and a dedicated neurological catheterization laboratory, which is accessible anytime to facilitate urgent and elective procedures. When a stroke code is activated post TAVI, a rapid neurological evaluation is performed followed by a brain CTA and a CT perfusion, if needed. Several scenarios can than unfold—in the presence of a moderate or severe stroke (NIHSS > 5) and a large vessel occlusion (LVO), the patient is considered for MT. In the presence of moderate or severe stroke and no LVO, the patient is considered for TT, if the bleeding risk is not prohibitive. In the presence of mild stroke (NIHSS ≤ 5), or in the combination of moderate or severe stroke, no LVO and prohibitive bleeding risk, the patient is managed with a CM.
In our local experience, of 18 patients with moderate or severe stroke only 7 underwent NI (39%). Of the remaining 11, three were denied therapy due to late diagnosis with little or no remaining penumbra at CT perfusion, five were denied due to the absence of LVO or a difficult to approach occlusion (PCA) and were not offered TT given a perceived high bleeding risk, and three were considered at high risk for any intervention.
Despite the small number of patients treated, several of our observations support the notion that meticulously selective NI to treat AISCT may be both safe and effective—(1) median NIHSS has declined dramatically after NI, (2) independent survival rate (mRS 0–2) at 3 months was significantly higher in NI as compared to CM in the moderate severity group, (3) median mRS score following NI for moderate severity stroke (median 1, IQR 0–2) resembled median mRS after mild stroke (median 1, IQR 0–3.25), and was numerically lower than mRS after CM for moderate severity stroke (median 3 IQR 1.25–5.75, p = 0.1).
Regarding the choice of intervention, as compared to MT, TT may be associated with both lower safety and reduced efficacy. Previous data suggest that TT after AISCT may be associated with an increased risk of major access site bleeding [15, 16]. In terms of treatment efficacy, considering that tissue-derived debris is often found in the assessment of embolized material collected from CEPD post TAVI [17, 18], MT targeting the retrieval of embolized material should be preferred over TT. TT should be considered in the absence of LVO or when access to MT is limited. Since only one patient in our cohort was treated with TT, we cannot offer any insights regarding the effectiveness of this strategy after AISCT.
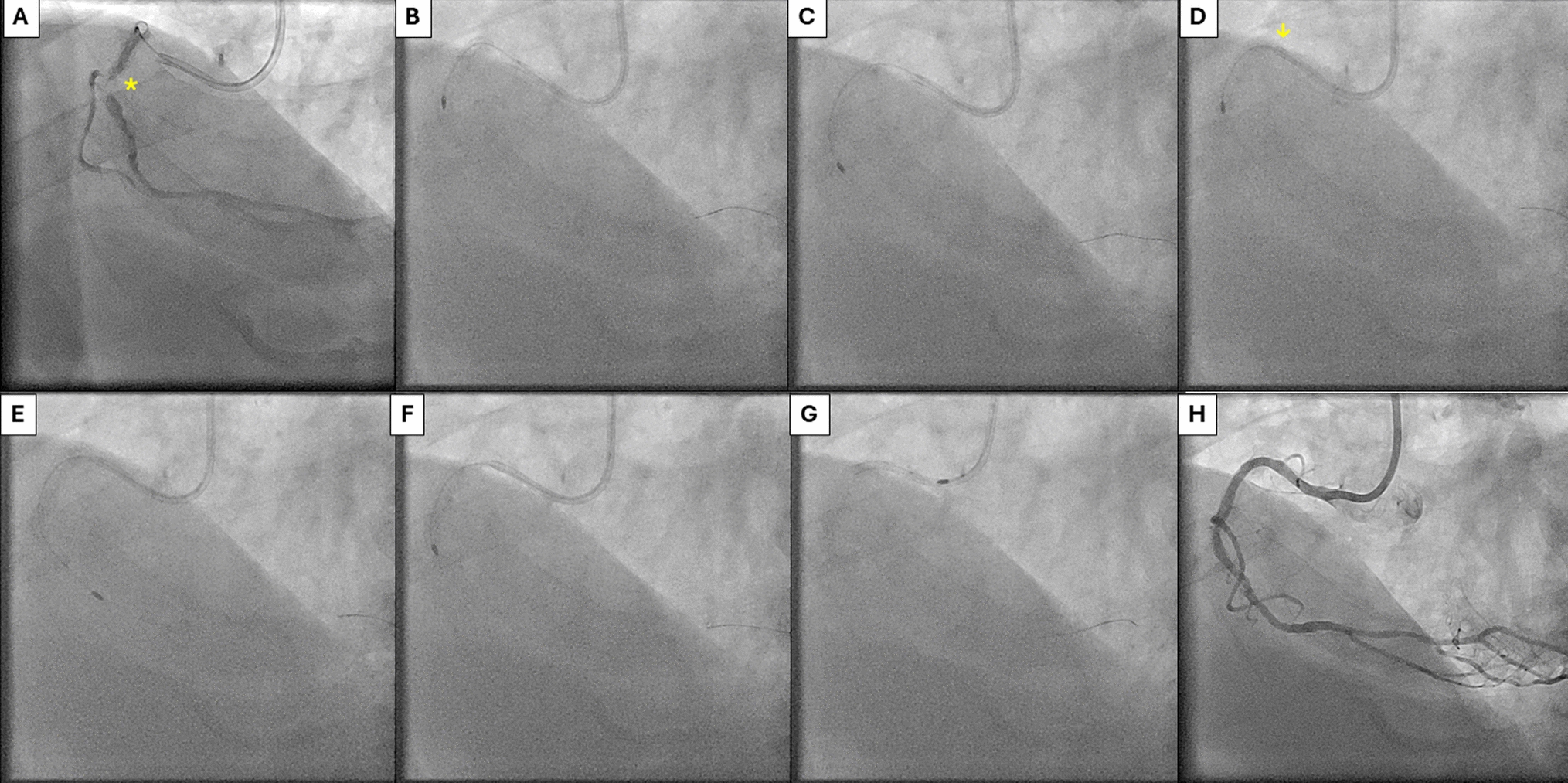
As reflected in our observation, timely diagnosis of AISCT is a major determinant of effective treatment. In this regard, several strategies may facilitate earlier diagnosis of AISCT. The first is adherence to conscious sedation (CS) rather than to GA during TAVI. While GA has not been identified as an independent predictor of AISCT [19], it may lead to an earlier diagnosis, occasionally while the patient is still on the catheterization table, and in turn to a rapid initiation of the diagnosis-imaging-treatment cascade. Furthermore, in the ASTRO-TAVI registry [15], GA was significantly more prevalent in the CM as compared to the NI group (14% compared to 38% respectively, p = 0.01), possibly implying that a rapid diagnosis of AISCT is linked to higher rates of intervention. In the current analysis, 4/7 patients in the NI groups were diagnosed with AISCT during or immediately after TAVI, all of whom underwent TAVI under CS. Of particular interest, is a case in which a 90-year-old female, who developed clear focal neurologic stigmata immediately after TAVI, underwent neuro angiography while still in the cardiac catheterization lab. Thrombus was aspirated from the left middle cerebral artery (MCA) with a good angiographic result. The symptoms improved rapidly, and the patient recovered with no significant disability.
The second factor in the chain of AISCT diagnosis is the availability of systematic evaluation by a neurologist. Recent studies have demonstrated that the detection of overt and covert CNS injury is directly related to the intensity of surveillance, with systematic examination by neurologists and routine CNS imaging yielding substantially higher event rates [20]. Furthermore, reported AISCT rates were found to be significantly higher in comprehensive stroke centers (CSC), as compared to non-CSC designated centers, suggesting that higher skills in stroke treatment and detection may promote higher rate of AISCT diagnosis [21]. It is therefore imperative to have a low threshold to assess all TAVI patients with a timely neurologic assessment, and to perform the necessary imaging when needed. Assuming 1.5% rate of 30 moderate/severe AISCT with a NI eligibility of about 50%, one patient in every 133 TAVI cases could benefit from a NI after an AISCT.
Limitations
Our study has several limitations: first, despite the absence of significant differences between the groups, there is a possible selection bias to CM in sicker patients. Indeed, three patients were deemed unsuitable for any intervention, all ending up with an unfavorable neurologic outcome. Second, some relevant data fields were not collected in our registry including CEPD use (low rate, approximately 5%), bicuspid aortic valve, and calcium score. Finally, the low number of NI may lead to a type 2 error in the interpretation of therapy related outcome and should be therefore considered as hypothesis generating.




Comments (0)