
Remember me



The research was carried out between January 2022 and January 2024 at the Cardiology Department of Ain Shams University Hospitals via prospective observational methods. Our registry included 336 patients of which fifty-four patients had severe rheumatic aortic stenosis. Patients were allocated into two groups; the first one included 54 rheumatic severe aortic stenosis patients and the other arm included 282 degenerative calcific severe aortic stenosis who were then propensity score matched into 54 cases. During the specified period, we performed TAVI in 54 cases representing 16% of the total 336 TAVI cases including both rheumatic and degenerative calcific pathologies. A convenience sampling approach was employed to find study participants. Patient outcomes were documented via the Valve Academic Research Consortium-3 criteria (VARC-3 criteria) [1], and patients were followed up for six months.
The inclusion criteria [according to the latest ESC guidelines of valvular heart disease (VHD)] [2] were patients above 65 years of age, fulfilling the criteria for rheumatic aortic valve by echocardiography according to the 2012 World Health Federation (WHF) criteria [3], concomitant rheumatic mitral valve affection, history of rheumatic activity, refusal by surgeons, symptomatic severe aortic stenosis (NYHA functional class, CCS grading, and syncope), aortic valve area < 1 cm2 or < 0.6 cm2/m2, high gradient AS (mean gradient > 40 mmHg or jet velocity > 4.0 m/s), low flow low gradient AS with impaired functions, low flow low gradient AS with preserved functions, and aortic valve annulus diameter ≥ 18 and ≤ 30 mm.
This study was authorized by the ethical committee of Ain Shams University, FMASU MD 127/2022. Each patient in the cardiology department at Ain Shams University hospitals received a thorough explanation of the process and gave their consent in a private setting. The primary researcher was the only one with access to the patient’s medical records, and the study was conducted in total secrecy. The participants were free to quit from activity at any time, and participation was entirely optional.
Preprocedural data analysisA diversified cardiac team comprising interventional cardiologists, cardiac surgeons, and imaging experts assessed the patients and categorized them into high, intermediate, or low risk groups. To estimate the risk of death for each patient, the European System for Cardiac Operative Risk Evaluation (EuroSCORE) II [4] and the Society of Thoracic Surgeons (STS) risk score [5] were calculated. A detailed preinterventional assessment was conducted on every instance. Every patient had an electrocardiogram, with the fundamental rhythm, axis deviation, PR interval, QRS morphology, and QRS duration recorded.
Patients had standard 2-dimensional B-mode and Doppler transthoracic echocardiography (TTE) prior to the procedure, and standard parameters were measured in compliance with guidelines provided by the American Society of Echocardiography [6].
The Osirix MD version software was utilized to process all computed tomography (CT) images. The measurements included the length of the membranous septum (MS) with values indexed to BSA (MSi), the diameter of the sinus of Valsalva, the height of the left and right coronary ostia (LMCA and RCA, respectively), and the calcification degree of the valve and basal septal calcification (Fig. 1) Moreover, thickness, commissure fusion, and calcification distribution were examined and verified using two- and three-dimensional computed tomography. Aortic valve calcification grading: There was no calcification in Grade 1, moderate calcification in Grade 2 (tiny, isolated areas), moderate calcification in Grade 3 (many, larger spots), and heavy calcification in Grade 4 (extensive calcification over the entire circumference) [7].
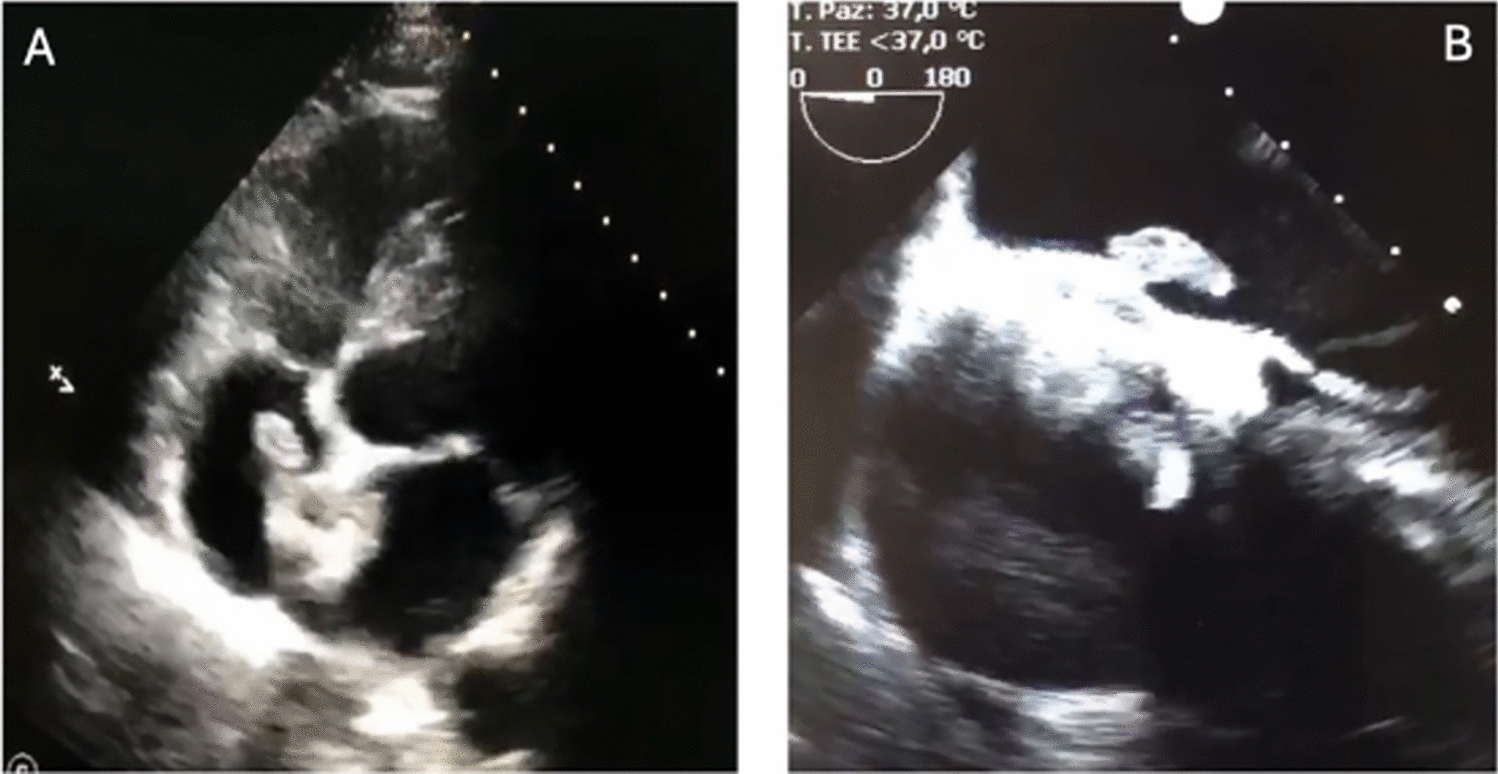
Fig. 1
Pre-TAVI CT assessment of rheumatic severe AS
Rheumatic mitral valve involved morphological features: (A) Commissural fusion; (B) thickening of the leaflets with or without calcification; (C) restricted mobility of the leaflets, which causes the anterior mitral leaflet to resemble a “hockey stick” or “doming” during diastole; and (D) thickening and shortening of the chords.
Rheumatic aortic valve involved morphological features: (A) Retraction of the leaflet margins; (B) fibrotic thickening; (C) commissural fusion; and (D) a triangular or rounded opening in systole.
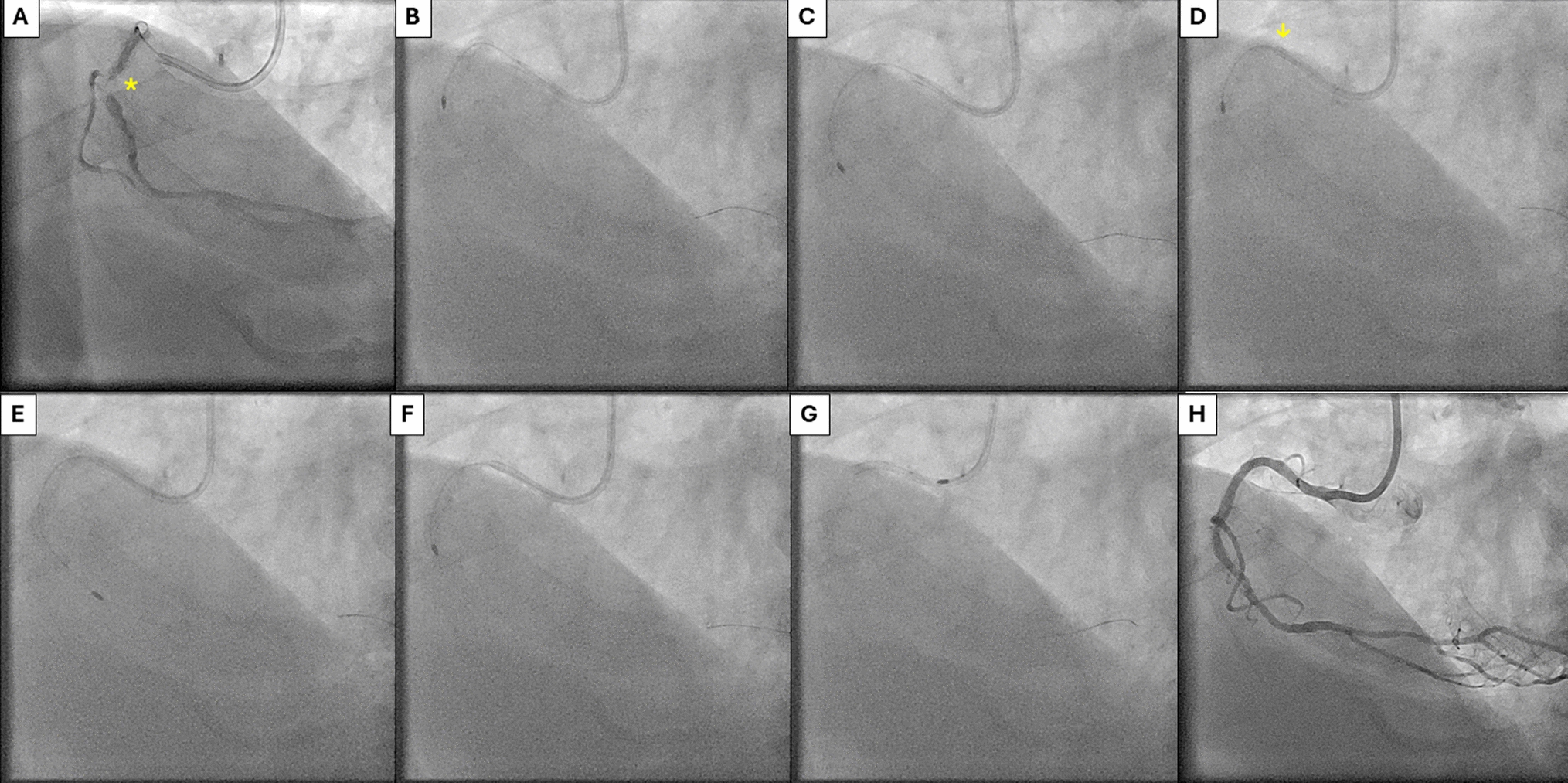
ProcedureStandard procedural steps for TAVI were implemented [8]. Valve options available were Evolut R™ (Medtronic, USA), Acurate Neo 2™ (Boston Scientific, USA), Sapien 3™ (Edward’s Life Sciences, USA) and MyVal™ (Meril life, India) (Fig. 2) Postimplantation balloon valvuloplasty was performed in patients with moderate AR or with a residual significant pressure gradient across the valve.
Fig. 2
Different TAVI platforms used in rheumatic AS
The depth of implantation was defined as the distance the between the native aortic annulus plane and the medial border of the implanted valve. The membranous septum length–implantation depth (ΔMSID) and the percentage of depth of implantation to the membranous septum (DIMS) were the two metrics used to evaluate the correlation the between the membranous septum and depth of implantation [9].
Postprocedural outcomesClinical follow-up, electrocardiogram (ECG), and transthoracic echocardiography were performed post-procedure with the same variables being followed up at hospital discharge, 30 days after device implantation and 6 months. Procedural complications were defined according to the VARC-3 criteria [1].
Statistical analysisStatistical analysis was done by SPSS v26 (IBM Inc., Chicago, IL, USA). Shapiro–Wilk test was used to evaluate the normality of the distribution of data. Quantitative parametric variables were presented as mean and standard deviation (SD) and compared between the two groups utilizing unpaired Student’s t test. Qualitative variables were presented as frequency and percentage (%) and were analyzed utilizing the Chi-square test or Fisher’s exact test. A two-tailed P value < 0.05 was considered statistically significant.
Propensity score (PS) weighting analysis was done to adjust for measured confounders between both groups regarding the demographic data (TAVI in rheumatic vs. TAVI in degenerative AS). Patients’ weights were derived from the PS weighting methods, in which each patient’s weight is the probability of that patient being assigned to the opposite treatment group. The balance between groups after overlap weighting adjustment was shown by reporting the weighted covariate means (or proportions) for the 2 groups being compared. We performed a propensity score matching between patients with rheumatic AS and without rheumatic AS who underwent TAVI, regarding the pre-procedural data collected including demographic data, ECG, echocardiography, and CT data.
Comments (0)