
Remember me
Distal shunts aim to achieve detumescence by establishing a fistulous connection between the corpus cavernosum and the glans penis. Distal shunts can be further characterized as “percutaneous shunts”— which includes the Winter shunt [9] (biopsy needle), Ebbehoj shunt [10].
(#11 blade), and T-shunt [11, 12] (#10 blade)— and “open” distal shunts including the Al-Ghorab [13] (excision of the tunica albuginia) and Burnett or Corporal Snake shunt [14] (Al-Ghorab with dilation).
Efficacy of distal shunts for erection times <48 h is somewhere in the 70% range, with rates of ED reported around 25% [9,10,11,12,13,14]. Distal shunt failure is likely due to the inability of a small shunt (particularly the Ebbehoj and Winter shunts) to accommodate the post-ischemic hyperemia, leading to new clot formation and occlusion of the shunt. More modern approaches— such as the T-shunt [11, 14] and the Burnett/Corporal Snake [14]— use the framework of old techniques with simple modifications to address the “small shunt” shortcomings.
Notably, there is discussion in the literature of periprocedural anticoagulation when preforming distal shunts, however this has not yet been included in guidelines [15,16,17]. The clotting cascade is activated after oxygenated blood is exposed to the incised tunica albuginea, which can lead to clot formation and subsequent blockage of the shunt [16]. Short term (5 days) duel antiplatelet therapy may allow the shunt to remain open for long enough to prevent priapism recurrence, but not long enough to create a permanent fistula resulting in long term ED [17].
Percutaneous distal shuntsPercutaneous distal shunts achieve fistulization between the glans and the corpora without the need of an open incision. Percutaneous shunts can be done at bedside with adequate local anesthesia (most often a dorsal and a ring block) or in the operating room if patient or surgeon prefers.
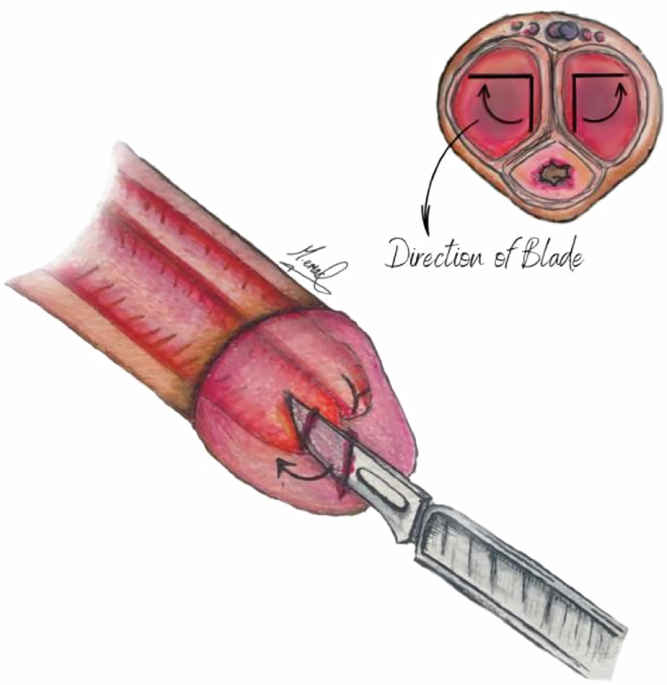
The T-shunt— named for the “T” shaped incision it leaves on the glans— was first described by Garcia et al. in 2008 [11, 12]. Similar to1974 Ebbehoj technique [10], the T-shunt involves inserting a blade through the glans of the penis. The T-shunt technique employs a 90° rotation laterally (i.e. away from the urethra) to create a “T”, and scalpel is then withdrawn to allow for evacuation of deoxygenated blood (Fig. 1). This procedure is first completed unilaterally, if the penis remains rigid or if priapism recurs within 15 min, then procedure can be repeated on the contralateral side. For patients with prolonged episodes of priapism (>2 days) or difficulty expressing old blood, dilation of the cavernosa in addition to the T-shunt technique can be considered [11,12,13]. Dilation with a 7 mm straight sound through the glans incision(s) to the crura/base of the penis (referred to as “tunneling”) creates an intracavernous tunnel to reestablish cavernous blood flow [11,12,13].
Fig. 1
T-shunt. A #10 blade is inserted through the glans into the distal corpora and rotated 90° laterally to create a shunt between the corpus cavernosum and the glans penis.
Multiple studies have reported that distal shunt surgery ±tunneling was successful as a treatment for priapism (80–94%), with a low complication rate and the potential preservation of erectile function (up to 62%) [11, 13, 18]. Reported success of the T-shunt with intracavernous tunneling appears to be dependent on duration of the priapism episode, proving less reliable in episodes lasting more than 48 h [18, 19].
Winter shuntThe Winter shunt is a percutaneous procedure in which a large-bore biopsy needle, such as a Trucut or Biopty gun, is used to create a fistulous connection between the glans penis and corpora cavernosa (Fig. 2) [9]. The Winter shunt has historically been a common initial approach after failed irrigation as it is simple to perform, can be done under local anesthetic, and comes with minimal complications [9].
Fig. 2
Winter shunt. Large biopsy needle is passed through the glans into the corpus cavernosum, creating a fistula between the glans and the corpus cavernosum.
Multiple retrospective studies have shown limited success of Winter shunting in adults,[20, 21]. A 2012 to 2014 case series found that 12 of 14 patients who initially underwent a Winter shunt subsequently required shunting with Al-Ghorab or Quackels approaches due to recurrence of the priapism— just a 14.3% success rate [21]. Other reported success rates range between 18 and 26% [21,22,23,24].
It is worth noting the Winter shunt is still of use in the pediatric population. Uzair et al. described a modified technique to treat pediatric priapism using two large bore, 16 gauge angiocatheters passed from the glans through the corpora cavernosa bilaterally with a 71–80% success rate in achieving detumescence and few reported long term effects on erectile function [23,24,25].
Open distal shuntsAl-ghorab shuntThe Al-Ghorab shunt— developed in 1981 by urologist Mohamed Mahoud Al-Ghorab— uses an open approach to create distal shunt between the corpus cavernosum and the glans penis [13, 14]. A transverse incision is made on the dorsal glans over the distal end of the corpora cavernosum, and deeper corpus tissue is dissected away from the tunica albuginea to reach the corpus cavernosum. A 5 × 5 mm circular cone segments of the tunica albuginea are excised from each corporal body, and once all the old blood is evacuated from the corpora, blood can flow freely from the corpus cavernosum to the corpus spongiosum (Fig. 3, Left).
Fig. 3: Open distal shunts.
(Left) Al-Ghorab shunt. Excision of a cone of tunica albuginia through a transverse glans incision creates a shunt between the corpus cavernosum and the glans penis. (Right) Burnett or Corporal Snake shunt.
Al-Ghorab has a proven success rate in achieving detumescence, with an approximate success rate around 74% [13]. Nixon et al. found that only 8% in patients who underwent an Al-Ghorab shunt primarily required reshunting [20]. Additionally, after failed percutaneous approach, successful detumescence for the Al-Ghorab technique was noted in 66.7% of patients [21]. There are limited studies that report rates of ED following Al-Ghorab shunts. A 2010 study reported on 7 patients who had undergone the Al-Ghorab shunt looking for outcomes on sexual function— one was lost to follow up, 4 were continued to be impotent and 2 had normal erectile function [19].
Burnett Shunt (“Corporal Snake”)The Burnett Shunt, also known as the Corporal Snake technique, is a modification of the AlGhorab [25]. After the circular core of the tunica albuginia is excised, 7/8 Hegar dilators are then inserted into the defect and advanced proximally several centimeters (Fig. 3, Right). The technique was coined by Arthur Burnett after he observed inadequate egress of thick, deoxygenated blood with standard techniques. Notable publication in 2009 noted 3 cases with successful resolution of ischemic priapism with 2/3 patients preserving their erectile function [14]. Notably, 1/3 patients had failed the traditional Al-Ghorab approach before undergoing the Corporal Snake modification [14]. A long-term case series published in 2013, reported an 80% detumescence rate. There were notably high rates of post operative ED in this study, with only 2/6 men with normal preoperative erections reporting recovery of partial erections postoperatively. Other complications reported included skin necrosis and intraoperative urethral injury [25].
Both the Al-Ghorab and Burnett techniques carry a risk of denervation of the glans penis due to the proximity of the incision to the dorsal nerve of the penis as well as urethrocutaneous fistulas [21, 26]. During the Al-Ghorab technique, advancing the dilators slowly with a slightly lateral angle can minimize the risk of concomitant urethral injury and subsequent urethrocutaneous fistula formation [13].
Comments (0)