
Remember me




A multidisciplinary, international writing group was established in which members were invited to contribute based on their previous work in the field; for example, a track record of relevant publication, or involvement in establishing local guidelines. In an attempt to reduce bias, attention was paid to ensuring not only multidisciplinarity, but also country of work and languages spoken. In addition to radiation oncologists, radiation therapists (RTT), a medical physicist and a radiobiologist; two patient representatives (AC and JD) were fully integrated throughout the entire process and were also included in the writing group. Guidelines, recommendations or similar were collected in languages the writing panel was capable of working with; i.e. the Italian [10], German [11], UK (Society of Radiographers) [12], French [13], Oncology Nursing Society (ONS) [14], International Society of Nurses in Cancer Care (ISNCC) [15], Dutch [16], and Belgian [17, 18]. Additionally, a translated Danish recommendation was added [19]. These documents were accessed with the assistance of colleagues within the ESTRO RTT committee, and the consensus of these documents formed the basis of these practical recommendations.
Given some national guidelines lack an evidence review and have evolved based on local practices, to provide an evidence-based foundation for the information contained within them, a literature search was conducted. The search strategy was compiled with the assistance of a subject librarian, and full details are included in the supplementary material. The literature included was limited to capture evidence from reviews, systematic reviews and meta-analyses of randomised controlled trials (RCT). The treatment of all cancer types using radiation therapy were included, with no exclusion criteria placed on the type of treatment or fractionation used. The screening process was conducted by two reviewers independently (EF and AOD), with any disagreement resolved via consultation with a third member of the writing group (PS). A total of 40 review papers were identified which was reduced to 27 after removing duplicates and screening for relevance. The MASCC guidelines published in 2023 [8, 20], with the linked systematic reviews [21,22,23,24,25,26,27] including meta-analysis were outside the scope of this paper’s search timeline but were subsequently added. These 29 papers were used along with the national guidelines to form the basis of the recommendations put forward by the writing group. If recommendations within several national guidelines were conflicting, this literary evidence was referred to drive consensus.
The recommendations from the guidelines were reviewed, and a minimum number of 3 guidelines giving the same recommendation was defined as an arbitrary threshold for a consensus. A summary of the recommendations of this panel deduced from these and the reviewed literature is presented in Table 1 in which the strength of the recommendation is rated in conformity with the ASTRO Clinical Practice Guideline Methodology Guide [28]. Additionally, the evidence was scored using a modified rating for the Quality of Evidence Levels (Table 2). Whenever in doubt or in case of a non-unanimous decision the next lower level was used for both scales.
Table 1 Summary of recommendationsTable 2 Quality of evidence (QoE) modified based on American Society for Radiation Oncology (ASTRO) Clinical Practice Guideline Methodology Guide [28] and strength of recommendation conforming with the sameRisk factors of RIDSeveral intrinsic and extrinsic factors have been identified to increase a patient’s risk of developing RID. Although there is little evidence of genetic predisposition to increased risk of RID, some rare conditions may lead to more severe degrees of RID. For example, a mutation of the ataxia telangiectasia mutated (ATM) gene causes ataxia telangiectasia syndrome, and these patients are more sensitive to radiation due to an inhibition in DNA repair [29]. Other pre-existing auto-immune skin conditions (e.g. lupus erythematosus and psoriasis) in some patients can flare up and extend beyond the irradiated area, requiring dermatological treatment. It must be noted, however, that RID is not absolutely predictable on the basis of intrinsic sensitivity, and other contributing factors must be considered [30]. For example, general patient factors such as smoking, and malnutrition can also increase or prolong RID.
Treatment-related factors which have been identified to increase a patient’s risk of experiencing a more severe degree of RID include anything which will increase the physical or biologically equivalent dose to the surface of the skin, such as higher total dose, boost dose, use of bolus, or lager treatment volume. Anatomical location of the treatment area will also influence RID risk. Due to the superficial nature of the target volumes, RID is commonly observed in patients undergoing radiotherapy with treatment volumes (and, as such dose) close to or encompassing the skin (i.e., breast, head and neck, anal, and vulvar cancer). Moreover, obesity leading to skin folds will also increase the dose to the skin in the folds, exacerbating RID risk in the area. Prolonged fractionation schedules longer than 4–5 weeks will also delay the onset of RID recovery. Finally, in addition to radiation therapy, systemic oncological treatments with chemotherapy or targeted therapy that reduce cell division or inhibit repair of DNA damage can also increase the severity or prolong the duration of RID.[7, 31,32,33,34].
Pathophysiology of RIDAnatomy and physiology of the skinThe skin consists of three layers; starting from the surface, the epidermis, the dermis and the sub-cutis (connective tissue). The deepest layer, the sub-cutis, forms a connection with the structures underneath the skin such as muscles and bones, and contains blood, lymph vessels, nerves and fat. The middle layer, the dermis, contains the hair follicles (invaginations of the epidermis), glands, blood vessels, sweat glands, and nerves. Although very thin (30–300 μm) and not containing any blood vessels or nerves, the most superficial layer, the epidermis, serves as protection and prevents moisture loss.
Within the epidermis, is the regeneration layer or stratum basale, which contains the stem cells that serve as a reservoir. Within the layers of the epidermis, specifically the horn forming layer and the horny layer (stratum corneum), the keratinocyte stem cells are transformed stepwise to horn cells. The horn cells are eventually lost [35]. Depending on the thickness of the skin, a cell from the epidermis takes between 12 and 48 days to migrate from the basal cell layer to the surface; referred to as the ‘transit time’ [36]. As a result of this ‘transit time’, it takes on average 30 days for the epidermis to be completely renewed. Acute radiotherapy skin reactions have their origin in the epidermis, whereas late effects are related mostly to changes in the vascular structures of the dermis, and can occur several months or years following treatment completion. Changes in pigmentation are correlated with acute reactions and, whist hypo- or hyperpigmentation may resolve over time, telangiectasia is permanent [37]. Other chronic events that involve the skin include radiation-induced morphea; a rare inflammatory condition caused by abnormal deposition of collagen. Radiation induced skin cancers can also occur as a result of vascular damage of the dermis; however, in the case of squamous cell carcinoma, the latency period can be as much as 20 years [38].
Radiobiology RIDSeveral studies examined the effects of fractionated radiotherapy on human skin in patients treated for prostate [39] and breast cancer [40, 41] with external beam radiotherapy. This work identified that early skin reactions are not the result of massive cell death (apoptosis) in the epidermis, but rather the consequence of continuing physiological loss of cells in the epidermis horn layer without the timely replacement of these cells from the basal layer due to radiation-induced cell cycle blockade [39]. This can be considered as a survival response to the radiation, as during cell division the stem cells are more susceptible to cell death from the radiation. These studies further identified differences between the repair capacity for late telangiectasia and that for erythema and desquamation [40]. These changes could be attributed to a modification in the immune and cell cycle pathways related to senescence [41].
In addition to the loss of epithelial cells, an inflammatory response develops in the skin that can cause soreness, swelling and erythema [42]. It is important to note that the term ‘erythema’ presents differently across different skin tones and can be misleading [43]. The British Association of Dermatology [44] states that erythema can be easy to miss in brown and black skin as the change in colouration can present as the skin becoming darker than the surrounding area. For some people with brown and black skin, the skin changes can present through pink, red, maroon, yellow, grey or purple skin colour changes [43]. It is important to understand the patient’s skin tone at baseline.
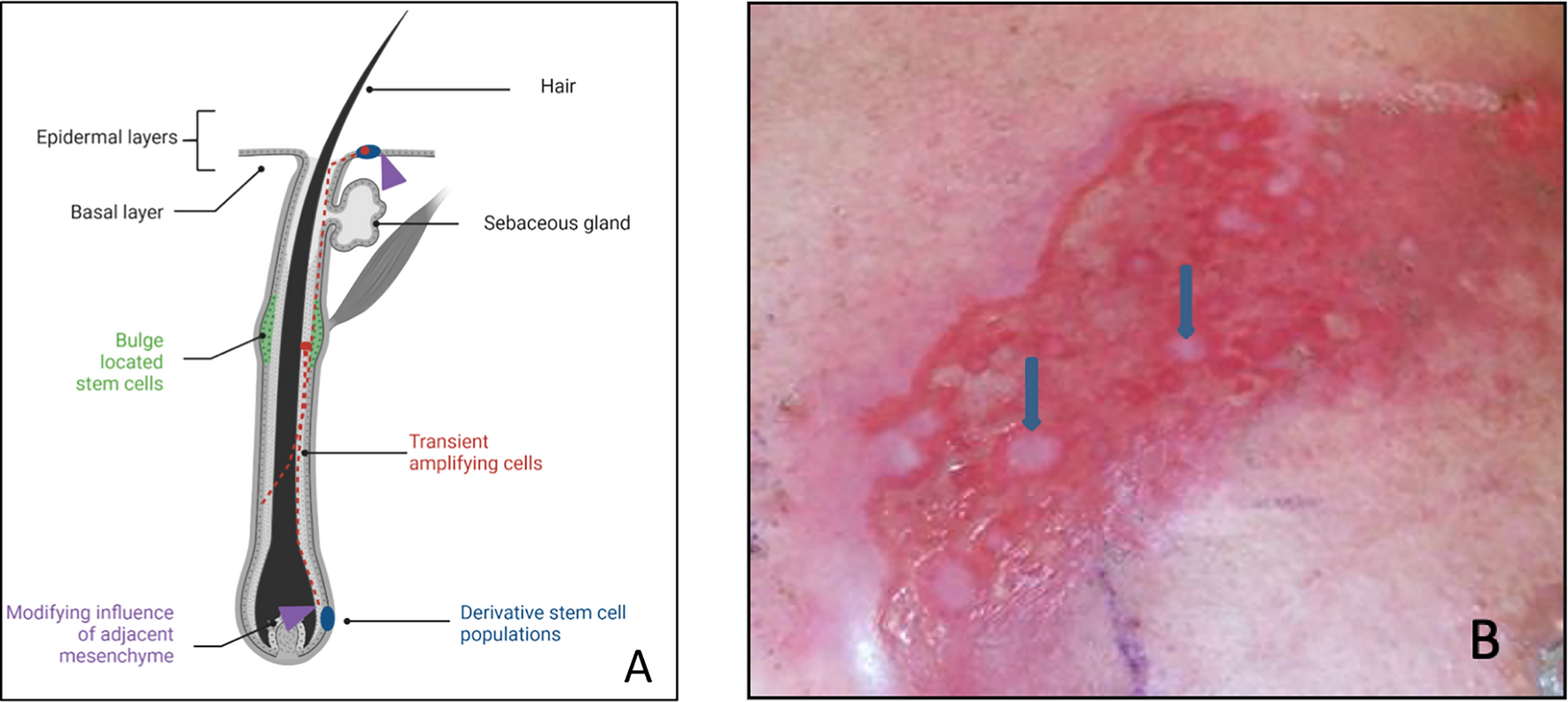
With increasing skin dose and/or time, complete denudation of the horn layer may occur, resulting in moist desquamation. The epidermis recovers through proliferation of cells from the stem cell compartment. The true stem cells are found in the bulge compartment of the hair follicle [45, 46]. From here, the stem cells can migrate down to the root of the hair follicle, or to the epidermis, the derivative stem cells in Fig. 1a. When moist desquamation starts to heal, the skin regenerates from the hair follicles with small islands of new skin that extend and coalesce (Fig. 1b). In the case of an imbalance of pro-inflammatory and profibrotic cytokines, chronic RID can manifest. This irreversible condition is characterised by a change in vascularity, pigmentation, and fibrous tissue [38].
Fig. 1
a Position of multipotent stem cells in the bulge compartment in the hair follicle root sheath. Derived lineages migrate to the skin surface to regenerate epidermal cells. b Regeneration of the epidermis in an area of epidermolysis. Islands of regrowth (arrows) derived from the stem cells of the hair follicles gradually coalesce
As detailed by Bennado et al. [38] other, rare chronic events have also been linked to RID. Only occurring in approximately 6% of patients previously treated with radiotherapy, radiation recall is a phenomenon which is poorly understood. Whilst the exact pathogenesis remains unknown, it has been postulated that radiation induced changes to the stem cells, along with DNA damage and oxidative stress are likely to trigger an acute inflammatory response at the original radiation site when a drug is administered months or years after the original treatment. The clinical manifestation of radiation recall is similar to that acute RID, and may include desquamation and pruitis.
Scoring RIDGrading and clinical assessmentOver the years several different systems have been developed to assign a grade reflecting the level of normal tissue damage, both in the acute and late setting [47,48,49]. Despite international efforts in standardization across all disciplines in oncology, we still see a range of scoring systems across Europe being used for the assessment of RID.
The Common Terminology Criteria for Adverse Events (CTCAE), current version 5, 2017 [50] includes both acute and late effects from treatment. Within the grades, specifically Grade 2 and 3, the impact on “activities of daily living” (ADL) is also considered, reflecting the patients’ quality of life. Whilst the CTCAE is the system adopted in the Dutch guidelines [16], the French [13] and Italian [10] guidelines have employed a slightly edited version; motivated by the need to consider the synergistic effects of combined therapies and the occurrence of “bio-radiation dermatitis”; e.g. experienced with the concurrent use of cetuximab [51, 52].
An alternative system is that of the EORTC/RTOG [49], recognized for use in both the Italian and UK guidelines [10, 12]. Although limited to targeting acute toxicity only, this system has been shown to have high rates of inter-observer variability when compared with other established systems [53]. Table 3 presents a comparison of these systems for RID.
Table 3 Comparison of WHO, EORTC/RTOG, CTCAE v5.0, and CTCAE (modified) for the scoring of skin toxicityThe use of photographs in the clinical environment may also provide useful supplementary information to monitor progression and/or response to interventions when needed, and their use is recommended by the panel. Figure 2 shows examples of the different grades of RID.
Fig. 2
Examples of the different grades of radiodermatitis
Whilst it is apparent that several different scoring systems are used in routine clinical care across Europe, consistent use of one single system amongst the multidisciplinary team within individual institutions is critical. Timing of the assessment should also be standardized; a point which is currently lacking in most guideline documents. In this regard, the UK guidelines recommend weekly assessment and grading [12]. Assessment of adverse events should also include reporting at baseline (i.e., prior to treatment commencing). Assigning a grade at this point is particularly important in specific clinical scenarios; for example, in the post-operative setting, or where reconstructive procedures have been undertaken, such as skin flaps or skin grafts. Furthermore, reporting at baseline also allows for responsible monitoring and appreciation of the progression of RID throughout the treatment course. At baseline assessment, it is important to evaluate intrinsic and extrinsic risk factors that may influence the frequency, severity, and duration of skin reactions. Professionals should be aware of altered skin reactions that may develop or be exacerbated by other therapies; for example, if patients receive concomitant chemo- or immunotherapy [54, 55] as well as the potential of a recall skin dermatitis [56]. Based on intrinsic factors, it is possible to stratify patients with a low, medium, or high risk of developing severe skin reactions, allowing for prompt intervention where required. Whilst there is a lack of high-quality evidence to inform risk stratification [7], machine learning methods are now being used to develop more eloquent predictive models for RID [57,58,59].
Patient involvement and self-assessmentWhilst these established scoring systems are useful, when scoring side effects that are often subjective, there is the potential to undervalue the impact on patients’ quality of life. In addition, there is a recognized lack of concordance between the grade assigned by the health care practitioner and that of the patient [60]. To overcome these concerns, separate quality of life scoring systems, such as the European Organisation for Research and Treatment of Cancer Core Quality of Life Questionnaire (EORTC QLQ-C30) [61], and patient reported outcome measures (PROMs) have been developed [62, 63]. Specific to RID (Table 4), the Radiation Induced Skin Reaction Assessment Scale (RISRAS) and the Skin Toxicity Assessment Tool (STAT) are commonly used [64]. Unique to these scales is the hybrid of both a PROMs component as well as a scale for scoring by the health care professional; thereby capturing both the objective and subjective domains, combined in a total score. Whilst the Italian [10] and Belgium [17, 18] guidelines do not mandate the use of the RISRAS, the value of this system, when used in combination with other classification systems, is recognised. Conversely, the Italian guidelines [10] refer to STAT as a valid tool to be used [65]. Another alternative tool is the Dermatology Life Quality Index (DLQI) [66]. This questionnaire measures the impact of skin disease on the patient’s quality of life, where each of the ten questions considers the impact over the previous week. This tool may also be supplemented with an additional illustrative version [67]; yet despite being validated, neither appear in many of the guidelines reviewed. Similar to the DLQI [66], the Skindex-16 rates skin conditions that have occurred in the previous week, with a 16-item patient completed form using numerical analogues scales and 3 subscales (14).
Table 4 Assessment tools for radiation induced dermatitis (RID), evaluating patient-reported outcomes measuresThe panel recommends involving the patient and evaluate the different options available [68] to incorporate patient reported skin reactions, during and after radiation therapy.
Prevention and management of RIDPrevention and general skin care managementPrevention of RID comprises the reduction of irritants and trauma to the skin, taking care during washing, with the application of topical agents during radiotherapy, as well as taking care during sun exposure and activities such as swimming. The overall recommendations based on the majority of guidelines and systematic reviews for general skin care management are listed in Table 5. As highlighted in the Dutch [16], UK [12] and Belgian [17, 18] guidelines, healthcare professionals need to be provided with clear instruction and adequate education to ensure skin care management is appropriate. Prior to RID becoming apparent, baseline assessment and stratification of risk factors is also encouraged. The UK [
Comments (0)