Study design
A full-body Thiel-embalmed human cadaver specimen from the University Medical Center Groningen (UMCG) Skills Center was used for the present post-mortem infection imaging study [22]. All post-mortem experiments were performed in duplo, using both legs of the cadaver specimen. The deceased had provided written consent for the post-mortem use of the body for research and education purposes. The post-mortem experiment was conducted at the Wenckebach Skills Center of the UMCG in accordance with the applicable law (“Wet op de Lijkbezorging,” Art 18, lid 1 and 19, BWBR0005009) and UMCG guidelines.
We performed surgery on the tibia and femur, applying a total of 16 VariAx 2 titanium 4-hole compression plates (Stryker, Kalamazoo, USA) for osteosynthesis, with four plates each on the left femur, left tibia, right femur, and right tibia. Each plate was partially covered with biofilm and incubated with either phosphate-buffered saline (PBS), vancomycin-IRDye800CW, [18F]PQ-VE1-vancomycin, or both vancomycin-IRDye800CW and [18F]PQ-VE1-vancomycin. A surgical debridement was performed, following the clinical recommendations for treating fracture-related infections as described by Metsemakers et al. [23]. At various time points, FLI and PET/CT scans were performed to detect and quantify bacterial infection on the implanted osteosynthesis plates before and after surgical debridement. A schematic representation of the procedures is depicted in Fig. 1. PET data was quantified in Bq/mL, and FLI in mean fluorescence intensity (MFI, arbitrary units (AUs)), per implant side. Subsequently, ratios were calculated between the biofilm-covered side and the sterile side of the osteosynthesis plate.
Bacterial culturing and biofilm formation on osteosynthesis plates
The Gram-positive bacterium Staphylococcus epidermidis (S. epidermidis) ATCC 35,984 was used in this study because of its high capacity to form biofilm [24]. Bacteria were cultured in Tryptic Soy Broth (TSB) supplemented with 2.5% glucose and 2.5% NaCl (TSB+). A day culture was prepared by inoculating 10 mL supplemented TSB+ at an OD600 of 0.05. After ± 1.5 h of incubation at 37 °C and 250 RPM, the now exponentially growing bacterial culture was used for the inoculation of the osteosynthesis plates at an OD600 of 0.05. Bacterial biofilms were grown on the above-mentioned titanium osteosynthesis plates, as shown in Fig. 1A. To this end, these plates were suspended from a stainless steel Kirschner wire (K-wire) at a height where half of each plate was submerged in TSB+ culture medium that had been inoculated with bacteria. The remaining half was not in contact with the medium to serve as a non-biofilm control. Each day, the osteosynthesis plates were moved to a container with fresh TSB+ medium (without bacteria) until sufficient biofilm had accumulated on their surface, which was the case on day 4. Macroscopically, the submerged side of the plates developed an off-white, fuzzy biofilm layer, indicating the presence of adherent bacteria. No biofilm was detectable on the plates’ side that had not been in contact with the bacteria-containing medium. For the in vitro experiments, larger osteosynthesis plates (SPS; Stryker Plating System) one-third tubular plate, 8 holes, l = 103 mm, and rectangular blanks were prepared by culturing in a rectangular petri dish, using sufficient culture medium (inoculated with S. epidermidis, or maintained in sterile fashion). The plates and blanks were placed on 0.8 mm stainless steel (SST) Kirschner wires, to minimize direct contact with the bottom of the petri dish. Each day, the plates were moved to a petri dish with fresh TSB+ medium until sufficient biofilm had accumulated on their surface, which was the case on day 4.
Production of PET tracer and NIR fluorescent imaging tracer
[18F]PQ-VE1-vancomycin was prepared as previously described [5, 20]. Vancomycin-IRDye800CW was prepared by Symeres (Groningen, The Netherlands) as previously described [13].
Incubation of the osteosynthesis plates with fluorescent and/or PET tracers
Once biofilms had developed (on day 4), the osteosynthesis plates were removed from the culture vessel and washed by suspending the osteosynthesis plate in sterile PBS with 0.1% bovine serum albumin (BSA) to remove planktonic bacteria and culture medium. BSA was added to the PBS to mimic the wound environment, and to minimize non-specific accumulation of tracer. After washing, the osteosynthesis plates were incubated with either [18F]PQ-VE1-vancomycin, vancomycin-IRDye800CW, a combination of both tracers, or PBS, for a total of 20 min at room temperature. Each osteosynthesis plate was incubated with 0.3 MBq · mL− 1 of [18F]PQ-VE1-vancomycin, and/or 0.14 µM of vancomycin-IRDye800CW in 10 mL PBS, or PBS alone (Fig. 1A). For the in vitro experiment, each specimen was incubated with 1 MBq of [18F]PQ-VE1-vancomycin in sufficient PBS to fully submerge the materials. After incubation, the osteosynthesis plates were washed twice in PBS with 0.1% BSA to remove any unbound tracer. The washing procedure consisted of gentle submersion in the washing container, whilst trying to minimize disruption of the bacterial biofilms. Thereafter, the plates were ready for use in the surgical procedure, or in vitro experiments.
Surgical procedure and data collection
The human cadaver leg was disinfected and draped. An anteromedial incision was made over the tibia, and the lateral side of the femur, exposing both bones. Four biofilm-covered plates (Stryker, Variax 2-foot broad straight plate, 4-holes, l = 35.5 mm x w = 8.5 mm) were placed on the tibia and four on the femur of each leg. The plates were fixed to the bone using a single VariAx 2 T10 bone screw (3.5 mm x l = 26 mm) on the non-biofilm side of the plates (Figs. 1B and 2). A separate incision was made over the proximal fibula and the bone was exposed. To investigate whether our FLI and PET tracers also detect clinical biofilms in the post-mortem model, a plate extracted from a patient who had undergone revision surgery for FRI was placed on the fibula (METc 2017/526). The patient suffered from a confirmed Staphylococcus aureus (S. aureus) infection. Subsequently, FLI and PET/CT were performed at fixed time-points during the procedure to determine the potential to detect bacterial biofilms with our [18F]PQ-VE1-vancomycin PET tracer, and to quantify the efficacy of routine implant debridement in the removal of bacterial biofilms using our fluorescent vancomycin-IRDye800CW tracer (Figs. 1C and 2). FLI was performed at different instances during the first ‘diagnostic stage’ of the procedure: prior to and after osteosynthesis plate placement and after closure of the surgical site using Ethilon 3 − 0 (Ethicon, Somerville, USA). Measurements were performed using a Quest Spectrum fluorescence imaging system (Quest Medical Imaging B.V., Middenmeer, The Netherlands), held at a standardized distance of 30 cm from the surgical field. The camera was set to a gain of 22.5 dB and exposure times of 400 ms and 1000 ms. The detection limit of the Quest Spectrum, used for detection of the NIR fluorophore IRDye800CW was previously determined to be approximately 10 nM under ideal conditions [25, 26]. Subsequently, low dose CT and ultra-high sensitivity (UHS) PET was performed with the osteosynthesis plates in situ and closed wounds. Measurements were performed on a Biograph Vision Quadra system (Siemens Healthineers, Knoxville, USA). The first PET/CT scan was performed for a duration of 30 min. At the second ‘debridement stage’ of the procedure, the wound was reopened. Surgical debridement with 3 L of 0.9% saline was performed mimicking the standard of care clinical debridement (Fig. 2). Flowrate of the saline solution was regulated by gravity, and a sterile gauze was used during the debridement to dislodge bacterial biomass from the osteosynthesis plates. Afterwards, FLI was performed to quantify the efficacy of routine debridement and to detect any residual bacterial biofilm. Subsequently, the wounds were closed. The second PET/CT scan was performed for a duration of 60 min, marking the end of the procedure. In total, the experiment was performed over a time period of approximately 8 h from the start of incubation of the implants with tracer until the last measurement.
Data analysis
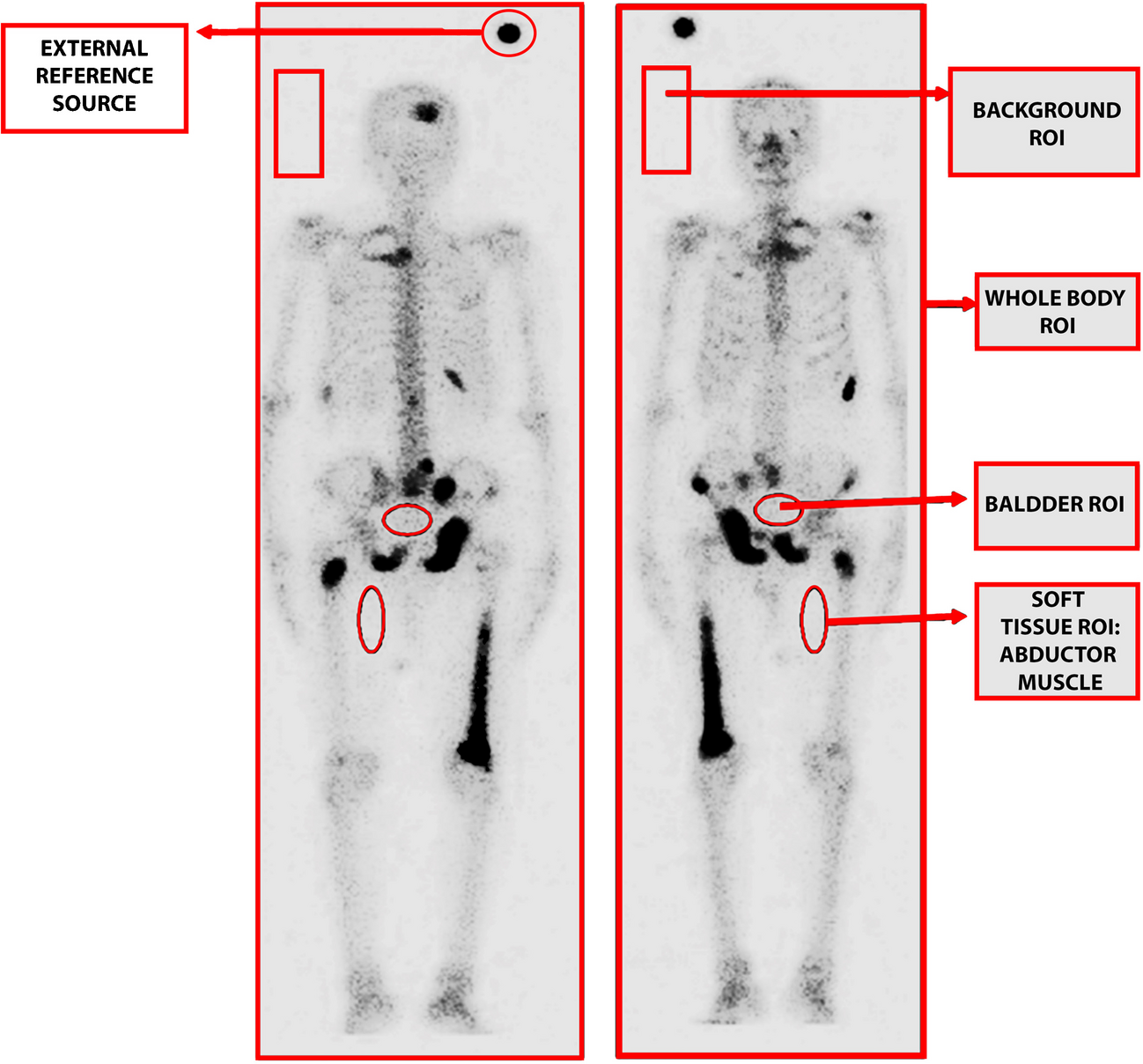
PET images collected were analyzed using Syngo.via software suite (version VB60 HF05, Siemens Healthineers, Erlangen, Germany). Volumes of interest (VOIs) were drawn (two with a diameter of 2.4 cm, encompassing each half of the osteosynthesis plate, and a third VOI was drawn with a diameter of 5.0 cm, encompassing the entire osteosynthesis plate) and exported as.csv files for further analysis. Fluorescence images collected with the Quest Spectrum fluorescence imaging device were analyzed using ImageJ (version 2.54d). Regions of interest (ROIs) were drawn and exported as.csv files (Fig. 3). Specifically, the osteosynthesis plates’ outline was traced using a polygon tool, making sure to differentiate the non-biofilm side from the biofilm-coated side. After debridement, this distinction was no longer visible, and the osteosynthesis plates’ midline was used as border between the non-biofilm side and the biofilm-coated side. The resulting files were imported into R Studio (version 2024.04.2 + 764, Posit PBC, Boston, USA). A non-parametric Mann-Whitney U test was performed to determine statistical significance, comparing accumulated signal (PET or FLI) pre- and post-debridement. Ratios were calculated by dividing target signal by non-target signal. A p-value of < 0.05 was considered to indicate statistical significance.




Comments (0)