
Remember me


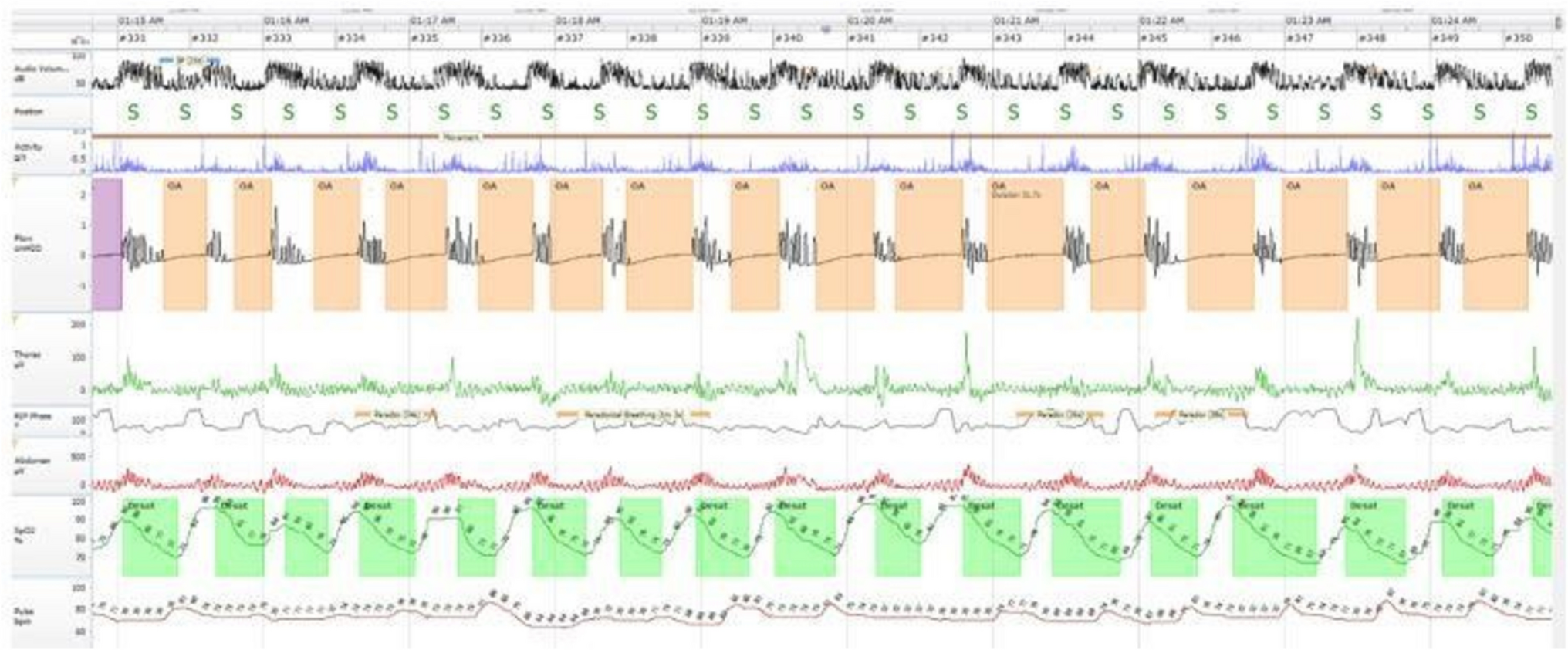




Obstructive sleep apnea (OSA) is characterized by recurrent episodes of complete (apnea) or partial (hypopnea) upper airway obstruction during sleep that causes arousal from sleep and/or a fall in oxyhemoglobin saturation (SpO2) [1] (Fig. 1).
Fig. 1
A home sleep apnea test recording showing intermittent pauses in airflow (OA) in Supine position with associated drops in SpO2 levels (Desat) and oscillations in the pulse rate. The snoring intensity achieves 100 dB, and breathing efforts during apneas are documented by the thoracic and abdominal belts showing that the apneic events are obstructive. OA, obstructive apneas
Obstructive apnea is characterized by an at least 90% reduction in airflow and it should be at least 10 s with inspiratory efforts of the upper airway muscles against the obstructed airway. For hypopneas, the reduction of the airflow should be at least 30% for at least 10 s. Moreover, these events should be associated with at least 3% drops in SpO2 levels and/or arousal [2]. OSA is diagnosed when the number of apneas and hypopneas per hour of sleep, an apnea–hypopnea index (AHI), at least 5 events/h or more on polysomnography (PSG) or home sleep apnea test (HSAT) in the presence of symptoms, such as snoring, excessive daytime sleepiness (EDS), or comorbidities such as hypertension, coronary artery disease [CAD], or stroke [3]. The cut-off level of AHI is 5 events/h for OSA diagnosis in the absence of symptoms [3].
Population studies in the early 1990s suggested that the prevalence of OSA was 9% in women and 24% in men, respectively [4]. Later studies showed an increased prevalence, 17% in women and 34% in men, which was attributed to increasing body mass index (BMI) in adult populations over the last 20 years [5]. The latest population-based study in Europe suggested that 61% of women and 84% of men had OSA in an unselected population of 1525 adults [6]. Globally, OSA has been estimated to affect more than 930 million adults [7].
Pathophysiology of Obstructive Sleep ApneaThe pharyngeal airway collapse is the key event in OSA and is considered to be a result of several malformations in the upper airway anatomy and its functions [8]. The airway collapses when the pharyngeal intraluminal pressure exceeds the forces that dilate the pharynx [9]. Reduction in the muscle tone and inadequate responsiveness increase susceptibility to OSA [9]. An oversensitive ventilatory control system (elevated loop gain) leads to increased fluctuations from the brainstem that reduces the partial pressure of CO2 in arterial blood below the apnea threshold [10], and consequently, a low respiratory arousal threshold may also cause obstructive events [11]. Other explanatory mechanisms contributing to OSA fluid shifts from peripheral tissues (lower extremities) to the neck, and airway edema [12]. Moreover, a neuromuscular dysfunction in the muscles controlling the upper airway tonus can also induce apneas. The most crucial muscle for this is the genioglossus, and sufficient contraction in this muscle seems to be important to avoid sleep apneas [13].
Clinical Symptoms of Obstructive Sleep ApneaSnoring loudly, EDS, fatigue, and observed apneas are the usual symptoms observed in patients with OSA. Other symptoms include nocturia, gastroesophageal reflux, and morning headache [14]. Of note, many patients, particularly the ones with cardiac diseases, do not report symptoms even though they may have very high AHI levels [15].
Treatment Options for Obstructive Sleep ApneaPositive Airway PressureContinuous PAP (CPAP) is the first-line treatment for patients with moderate to severe OSA (AHI ≥ 15 events/h) in the absence of symptoms, but it is also recommended for the treatment of mild OSA patients (AHI 5–15 events/h) when EDS or other comorbidities exist [16, 17]. CPAP titration is usually performed in sleep laboratories under attended PSG monitoring. Autotitrating PAP (APAP) is another commercially available treatment option [18]. Auto-titrating PAP devices are preferable for OSA patients, who have obstructive events in the supine position (positional OSA), and those with OSA during REM sleep [19]. It has been suggested that home APAP titration is effective as in-lab CPAP titration [20].
Upper Airway SurgeryAdenotonsillar hypertrophy is the main cause of pediatric OSA, and adenotonsillectomy is the first choice of therapy in children and young adults with OSA [21]. Nasal obstruction due to septal deviation may also lead to hypopneas [22]. Septoplasty or conchotomi can be thought in certain cases, and these surgical interventions may also be considered for patients who do not tolerate CPAP treatment due to nasal problems [19]. Uvulopalatopharyngoplasty was often used in the early 1980s and 1990s with good effect on snoring, but later studies suggested that those individuals at at high risk of developing silent apneas [19].
NeurostimulationHypoglossal nerve stimulation is a therapeutic option for patients who do not tolerate CPAP treatment [23]. It is a pacemaker-like device, that stimulates the hypoglossal nerve and protrudes the tongue, opens the pharyngeal airway, and consequently, maintains the upper airway patency. This treatment may reduce AHI by roughly 70% [24].
Lifestyle Interventions and Medical/Surgical Weight LossThe most important intervention for effective treatment in OSA patients with comorbid obesity is weight management. Weight loss may decrease the needed pressure levels of PAP in patients with sustained OSA, which is also crucial [25].
Positional TherapyPositional therapy has been developed to stop patients from lying in the supine position, when OSA is position-dependent [26].
Drug TreatmentThere is yet no established drug treatment for OSA, and a combination of noradrenergic and antimuscarinic drugs has been proposed [27]. In a recent RCT, it has been shown that the combination of atomoxetine plus oxybutynin improved the upper airway collapsibility, and decreased the arousal threshold [28].
Oral Appliance TherapyTongue-retaining devices (TRD) and mandibular advancement devices (MADs) are the commonly used oral appliances. The MADs are more frequently used, particularly in patients with mild OSA and in those who do not tolerate CPAP [19]. The MADs are not as effective as the PAP devices but may be beneficial in holding the mandible in a forward position, thus, avoiding the collapse of the upper airway muscles [29].
Since the introduction of the first commercially available intraoral devices for the treatment of OSA in the 1980s [30], there has been a markedly growth in the development of various MAD models [31]. The practice parameters for the use of oral appliances were first published by the American Academy of Sleep Medicine (AASM) in 1995 [32].
Tongue Retention Devices (TRDs)TRD was first described in 1982 [33]. It is an appliance that covers the lower and upper jaws. In its lingual part, there is a compartment that pulls the tongue slightly forward. When the tongue is placed inside the appliance, negative pressure is created, holding the tongue in place throughout the night [33]. TRD is designed to prevent the tongue from collapsing backward into the airway during sleep.
A meta-analysis study by Chang et al. shows that using TRD effectively reduces obstruction in the oropharyngeal region, resulting in a 53% reduction in AHI on average, increase lowest oxygen saturation by 4.1 oxygen saturation points, decrease oxygen desaturation index by 56% and decrease Epworth sleepiness scale scores by 2.8 points [34].
Mandibular Advancement DeviceTreatment with an MAD aims to keep the upper airways open during sleep by reducing its resistance and minimizing the frequency and duration of apneas, hypopneas, and snoring events. These devices work by advancing the mandible forward, which in turn helps to stabilize the pharyngeal structures, preventing airway collapse and obstruction. The degree of mandibular advancement is a critical factor in the effectiveness of appliance therapy for OSA treatment [35,36,37,38]. For patients with severe OSA, a greater advancement of the mandible has been shown to result in better treatment outcomes [39]. However, a meta-analysis conducted by Bartolucci et al. found no evidence that protruding the mandible more than 50% of the maximum advancement provided any additional benefit [39]. It is, therefore, recommended to "titrate" or adjust the degree of mandibular advancement individually to achieve the optimal therapeutic effect subjectively for each patient. It is important to be cautious with extreme advancements (e.g., 75% of the maximal protrusion) as the incidence of side effects tends to increase at higher degrees of the mandibular protrusion [38].
MAD TYPESMADs are in various designs (single-block or two-block, prefabricated or customized) and materials (acrylic, thermoplastic, or combination) to suit the specific needs of patients [40]. The customization of MADs involves tailoring the device to the patient's oral structure and physical requirements, optimizing its effectiveness and comfort.
Prefabricated MADsPrefabricated MADs, which come in standard sizes and shapes, may be less comfortable for some patients. Their lack of customization can lead to difficulties in retaining a stable mandibular protrusive position during sleep, potentially reducing their efficacy in treating obstructive sleep apnea [41].
Custom-made MADCustom-made MADs have several advantages over prefabricated ones. These MADs are produced by conventional impression or digital scan methods taken from the patient. Custom-made MADs, offer a more personalized fit, which is associated with increased patient-reported comfort, better range of mandibular protrusive movement, and higher therapeutic effectiveness in treating obstructive sleep apnea [41].
Custom-made MADs can be produced in non-adjustable, monoblock (one-piece appliance) (Fig. 2) versions or adjustable, duoblock (two-piece appliance or biblock) (Fig. 3) [41].
Fig. 2 Fig. 3
Fig. 3
Duoblock MAD/ Adjustable two-piece device
Non-adjustable MADs are fixed in a predetermined protrusive position and remain unchanged during treatment. In contrast, adjustable MADs offer the option of progressive advancements or titration (titration process), allowing for incremental adjustments to the mandibular advancement to achieve the best treatment efficacy and patient comfort.
There are different kinds of coupling mechanisms, such as; elastic straps, lateral fins, bars, telescopic rods, springs, and tube connectors among others. Each coupling mechanism has its advantages and limitations, and the choice depends on the specific requirements. The mechanism allows for controlled advancement of the mandible in small increments to achieve specific treatment objectives. The mechanism should be capable of advancing the mandible at least 5 mm forward from the starting position [38]. This range is important for achieving the desired therapeutic effect [35]. The mechanism also allows for precise adjustments in increments of 1 mm or less of the mandible's position. The initial position of the mandibular protrusion mechanism should be at least 50% of the patient's protrusive range [38, 42, 43].
Monoblock and duoblock are still the subject of discussion among dentists in terms of their advantages and disadvantages. The biggest expectation of dentists from the MADs is improvement in AHI and minimum oxygen saturation. A 50% decrease in AHI value after treatment compared to pre-treatment is considered a success [38]. In addition to the success of the treatment in the selection of the appliance, the cost of the treatment is also important for the patients and the physicians.
Production MethodIn a meta-analysis study, custom-made and ready-made MADs were compared, and custommade MADs were found to have a significant effect on AHI [44]. Moreover, custom-made MADs are more advantageous in terms of patient comfort and compliance compared to prefabricated MADs [45].
Monoblock vs Duoblock MADsIn a randomized controlled trial (RCT) by J. Zhou et al., a one-piece monoblock appliance and a 2-piece SILENT NITE® (GlideWell Laboratories, Newport Beach, CA, USA) appliance were compared. Although both appliances decreased the AHI by more than 50%, the monoblock appliance was found significantly more successful [46]. In a systematic review and meta-analysis by Hiroyuki Ishiyama et al., the efficacy of monoblock and duoblock appliances was compared [47]. Both of them showed a serious decrease in the AHI value, but the monoblock appliances were found to be more successful. In the study of Lee et al. [48], the efficacy and patient compliance of the monoblock and trinket appliance were compared. PSG records were obtained from the patients before and during the third month of treatment. According to the conclusion of the study, it was found that patients using monoblock MAD had a significantly higher response rate. On the other hand, the study found that patients using duoblock MAD had a significantly higher rate of compliance at the one-year mark compared to those using mono-block MAD. This suggests that patients using duoblock MAD are more likely to use the device consistently and effectively as prescribed for one year. These results highlight an interesting contrast between the two MAD types (mono-block and duoblock) in terms of their short-term effectiveness (response rate) and long-term user engagement (compliance rate). Mono-block MAD showed better short-term outcomes in terms of symptom relief, while duoblock MAD showed better long-term compliance in terms of patient compliance [48]. Notwithstanding, according to a meta-analysis, there is evidence that monoblock MADs are more effective at reducing AHI and improving minimum oxygen saturation compared to duoblock MADs [49].
Side EffectsMADs can have several potential side effects, including: Jaw muscle pain, temporomandibular joint (TMJ) discomfort or pain, tooth pain or changes in tooth alignment, irritation of the oral mucosa (soft tissues inside the mouth), dry mouth, increased salivation, vomiting or gagging, occlusal changes [43, 50]. Of note, these side effects can vary in severity and individual response. These side effects may be temporary or permanent, and to minimize them, it is important to perform an occlusal stabilisation. Moreover, there are many cases where OSA is seen together with bruxism. In addition, the use of an occlusal splint before MAD treatment has shown to minimize complications and side effects of the MADs, and this is particulary important when OSA and bruxism coexist [51, 52]. In a study conducted by Tegelberg et al., it was observed that respiratory disorders were significantly reduced in treatment with both duoblock and monoblock appliances [53]. At 1-year follow-up, a greater reduction in AHI values was seen with treatment with the duoblock appliance. however, it was found that treatment related adverse events were higher among duoblock users and that patients had higher rates of discontinuation [53]. In another study by Isacsson et al., mono-block and duoblock MADs had similar side effects [54]. Finally, in a study by Tuula Palotie, et al., it was shown that MAD treatment was more likely to be successful in patients who used occlusal splint before the start of MAD Therapy [55].
Recommendations for minimizing and preventing side effects associated with MAD use include:
1.Principle of keeping occlusion stable:
In the morning, the patient wears the stabilization splint and applies a warm massage. Performs biting exercises for 10–15 min [56, 57].
Circular massage is applied to the masseter and temporalis muscles. Thus, the jaw finds its normal centric occlusion position. If these are insufficient, the patient chews gum [56, 57].
The idea that wearing MAD will cause tooth movement is wrong. Because the alveolar stimulation that occurs during the hours when the patient is not wearing the appliance is sufficient to prevent tooth movement in any direction. It has been shown that it should be worn for 8 consecutive days without removing it from the mouth for any tooth movement to occur [57].
Doing isometric exercise (helps relax the lateral pterygoid muscle): The patient opens the mouth halfway and provides resistance to the opposing jaws with the finger. Patient tries not to close the mouth for 6 s against the resistance.
This movement is repeated 6 times [57].
2.Physical therapy; For the management of pain in the masseter muscle in the morning; Repeated circular massage for 6 s followed by 6 chin movements. Additionally, used in combination with a stabilization splint during the day [58].
3.Pharmacotherapeutic treatment: Use of NSAI once a day for three or four days in combination with a soft diet and ice massage [57].
4.Prosthetic application: If the problem is still not resolved, reduce the forward position of the mandible. Not using the appliance for a while or using it every 2 days
Treatment CostCustom-made appliances are more expensive than prefabricated ones, as they are made in the laboratory and require dental impressions or scans from the lower and upper dentition of the patient. Prefabricated appliances, such as “boil and bite’’ or thermoplastic appliances are cheaper than custom-made appliances. According to the findings of a study by Isacsson et al., both monoblock and bibloc appliances show comparable efficacy in achieving the intended treatment results [54]. In addition, for one year, the cost of using the duoblock appliance was higher compared to the Monoblock appliance. According to this information, although both appliances give similar results, the financial investment required for the duoblock treatment option is higher. Consequently, for patients seeking a more cost-effective option, may turn to the monoblock appliance, provided its efficacy is compatible with desired treatment goals [54].
Comments (0)