
Remember me

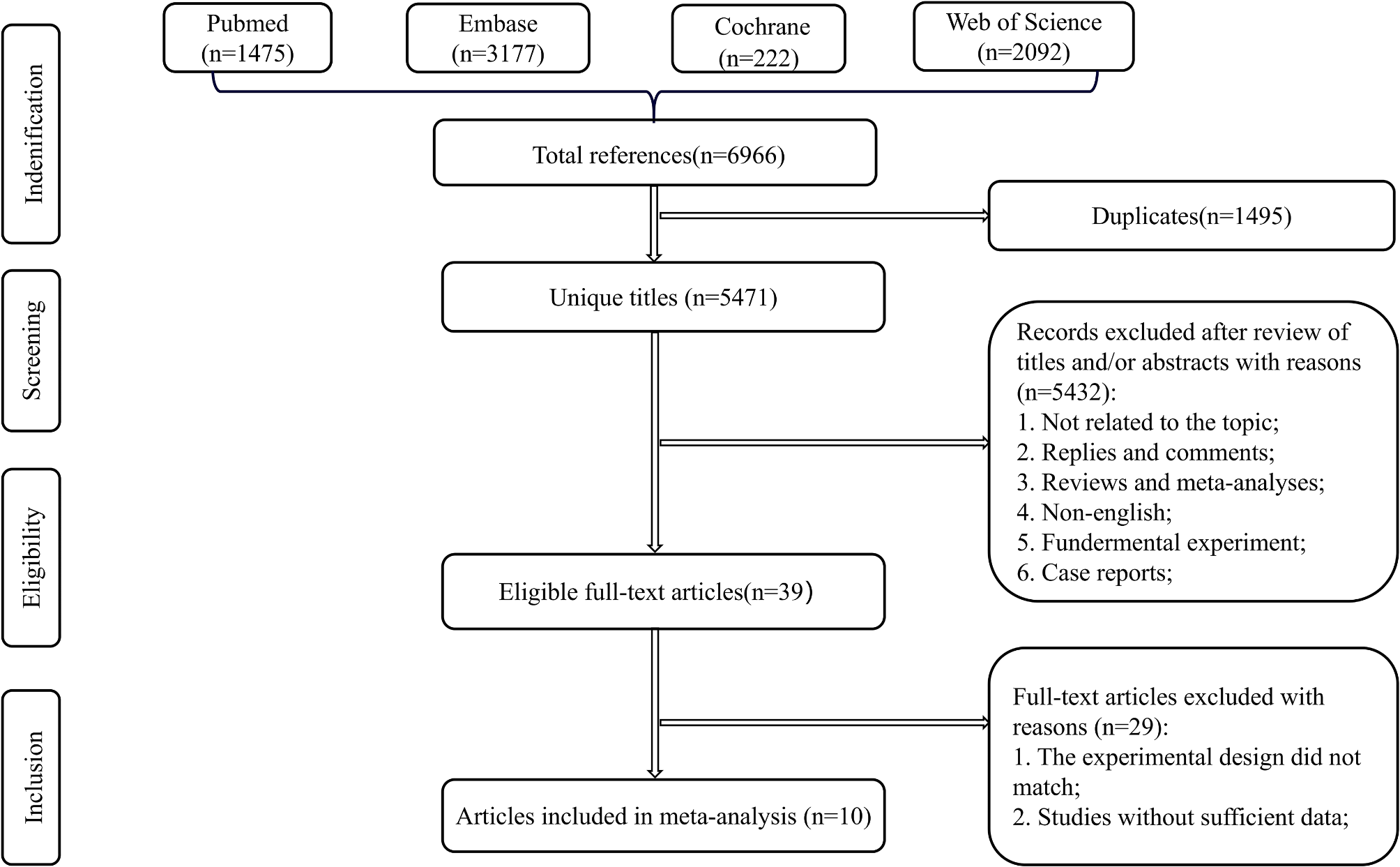



The most prevalent cause of valgus arthritic knees is osteoarthritis; however, they can also occur in people with rheumatoid arthritis, post-traumatic arthritis, and metabolic bone disease [2]. It is a complex entity with characteristics such as patellar malalignment, femoral and tibial metaphyseal valgus remodelling, hypoplastic lateral condyle, external rotation deformity of the tibia, and lateral tibial plateau bone loss [2]. Furthermore, it is also frequently observed that contracture of the lateral soft tissues, specifically the popliteus tendon, lateral collateral ligament (LCL), posterolateral capsule, and posterior cruciate ligament, has occurred [2]. These contractures are infamous for causing postoperative knee instability and are the primary cause of patellofemoral mal-tracking and lateral patellar subluxation [19]. The MCL becomes evidently lax or even rendered non-functional in cases of extreme valgus deformity. It is more difficult to achieve a well-balanced knee after TKA because of all these issues.
Based on the degree of soft tissue involvement and the severity of the deformity, valgus knees are usually categorized into three classes [15]. While 15% and 5% of patients, respectively, have moderate (Grade II) and severe (Grade III) deformity, the majority of patients have Grade 1 deformities. The medial collateral ligament is functionally elongated, the lateral structures are contracted, and the mechanical axis deviation is between 10° and 20° in moderate valgus deformity; in severe valgus deformity, the mechanical axis deviation is greater than 20°, the lateral structures are tight, and the medial stabilisers are not functional.
Historically, the primary objectives of knee replacement surgery are to achieve a stable joint and a neutral mechanical alignment in the coronal plane [20, 21]. In order to prevent early implant loosening and accelerated polyethylene wear, the gold standard was to create a favourable biomechanical environment for the implant by achieving a balanced load distribution between the components [21]. Surgeons have found it difficult to consistently obtain the best alignment and implantation of components, and the primary cause of failures with total knee arthroplasty is surgical errors [22, 23]. In 7% of cases, a mechanical axis deviation of 9 degrees was found in a study on conventional total knee arthroplasty, and in 34% of cases, it was over 5 degrees [24]. Conversely, research has demonstrated that robotic surgery produced outstanding alignment and placing of the implants, with errors as low as 1 to 3 degrees of neutral alignment [24, 25].
The biggest advantage of modern robotic-assisted TKA lies in its soft tissue algorithms, which allows surgeons to objectively evaluate the soft tissue envelope at the start and throughout surgery in a more robust and reproducible method. In addition, the precise amount of tightness and its location at the specific range of motion can be identified and quantified. Thereafter, necessary releases can be performed stepwise with objective feedback per release, allowing the surgeon to confirm if the releases are adequate to resolve any residual tightness.
In this series, as part of exposure, the senior author routinely released the lateral capsule from the anterolateral aspect of the tibial plateau and the iliotibial band from the Gerdy’s tubercle. The need for additional releases was decided after evaluation of the soft tissue envelope and performed with multiple ‘inside-out’ stab incisions of the iliotibial band and LCL as described by Ranawat et al. [15]. If gaps were still unbalanced as shown on the navigation screen, then the PCL and posterolateral capsule were released accordingly. In all cases, the popliteus was preserved and the femoral insertion of the LCL was maintained. With the use of the navigation function along with its soft tissue algorithms in robotic-assisted TKA, excessive lateral soft tissue release and overcorrection of the patient’s preoperative deformity were avoided.
In conventional TKA, the entry point for the intramedullary rod can be more medial in valgus knees and identifying this intraoperatively can be challenging. With the aid of the navigation function in robotic-assisted TKA, there is no need for the use of these rods as landmarks are marked virtually. Furthermore, previous hardware obstructing entry of these intramedullary rods need not be removed. Certainly, another advantage of the robotic-assisted TKAs is the ability to plan bony cuts prior to execution. This provides the opportunity to adjust bone cuts within acceptable boundaries to balance the soft tissue envelope in lieu of excessive releases. Finally, with the robotic-assisted arm, it is easier to execute bone cuts precisely.
Fig. 1
Case 02. (a) and (b): Preoperative clinical photograph and long-leg radiograph with severe valgus deformity of the right knee and a HKA of 36.5°. (c) and (d): Postoperative clinical photograph and long-leg radiograph with corrected deformity and a HKA of 1.9°. The posterolateral defect on the tibial plateau was addressed with autologous bone graft and screws. HKA: Hip-knee-ankle angle
Fig. 2
Case 05. (a) and (b): Preoperative clinical photograph and long-leg radiograph with moderate valgus deformity of the right knee due to extra-articular deformity from a malunited femur fracture. The HKA was 14.8°. (c): Postoperative long-leg radiograph depicting a corrected HKA of 0.01°. Previous hardware was not removed. HKA: Hip-knee-ankle angle
Fig. 3
Valgus and varus laxity on initial assessment of case 5. Initial knee examination reveals a grade 2 medial collateral ligament laxity, HKA of 14.8° and a range of motion of 15°- 110°
Fig. 4
Valgus and varus laxity at final assessment of case 5. Laxity have been well addressed. Intraoperatively the primary surgeon decided for a tibial cut of 2° varus. A size 10 PS insert was used. No lateral release was required. Resection thickness error of 1 mm. Final HKA was 0.1°and range of motion was 0°-120°
Table 1 Preoperative and postoperative clinical dataTable 2 Perioperative complicationsTable 3 Forgotten joint score and satisfaction scoreHowever, robotic-assisted TKA is not without its flaws. Higher costs, the need for additional pre operative imaging with trackers, pin site complications such as infection and risk of fracture both intraoperative and postoperative. All these should be considered prior to deciding the best surgical method suited for each individual patient. An ongoing study by Filippo Migliorini et al. on robotic- assisted total knee arthroplasty in clinical practice may help to conclude if all these said advantage of robotic- assisted TKA are true [11].
LimitationsThe main limitation of this paper is that it is a case series with low numbers. However, moderate and severe valgus deformities are not common entities, especially in developed countries. The experience and results presented here would still be useful for education and knowledge. Second, patients with similar deformities who underwent conventional TKA were not included and thus, surgical modality cannot be objectively compared. Finally, there is no long-term survivorship data in this series. However, it has previously been demonstrated how long implants with proper alignment and balanced gaps last [26, 27]. Larger data and longer follow up will be required to better understand the role of robotic assisted surgery in moderate and severe knee deformity.
Comments (0)