The first paper on G‑POEM was published in 2013 [11]. G‑POEM is a relatively new and moderately effective therapeutic modality for refractory gastroparesis. Gastroparesis is often difficult to treat because its pathogenesis is complex and incompletely understood. We published the first paper on the short-term outcomes of G‑POEM in our initial set of 16 patients about 8 years ago [12]. Since that time, several studies on short-term outcomes have been published with different rates of clinical efficacy ranging from 60 to 80% [6,7,8,9,10,11, 15,16,17,18,19,20,21,22]. The experience of a surgeon is one of the most important factors related to the outcome of a surgical procedure [14]. It is interesting to compare the short-term outcomes of G‑POEM performed by the same submucosal endoscopist early in his experience with a procedure and after years of practice with the same procedure in a different institution. To our knowledge, this is the first report of such a study.
The overall clinical success rate of 81%, with varying degrees of improvement in each domain of the cardinal symptoms, is similar between groups A and B, despite 8 additional years of endoscopy experience between groups A and B. The 80% clinical success rate in short-term follow-up is consistent with studies reported earlier in the literature [12, 15,16,17,18,19,20,21,22]. Interestingly, this finding indicates that there is a separate factor determining efficacy that has not changed over this 8‑year period.
First, the efficacy of G‑POEM may largely be determined by the selection of patients. Selection criteria have not significantly changed or improved since the outset of G‑POEM. Two prior studies identified obesity, a long duration of gastroparesis, and frequent use of psychic and pain medications as being associated with unsuccessful G‑POEM outcomes [9, 24]. However, standardized cut off values for body mass index (BMI), duration of disease, or medication exposure have not been established; therefore, such factors have not been used for patient selection before the G‑POEM procedure. In another previous study, our group analyzed proximal and distal gastric retention in gastric emptying scintigraphy and tried to identify the best candidates for G‑POEM; this preliminary study suggested that the proximal-to-total T½ ratio may represent an important patient selection factor for G‑POEM [23]. However, we need to study a larger sample size to validate it.
Unlike esophageal achalasia, where a tight esophagogastric junction predicts a good outcome after peroral endoscopic myotomy (POEM) [25, 26], a tight gastric outlet may not predict a good outcome after G‑POEM. One recent study concluded that endoscopic findings, such as the degree of pylorospasm and the amount of bile or food in the stomach, do not predict G‑POEM outcomes [27]. Therefore, at this time, there are no methods that reliably predict the outcome of G‑POEM before the procedure [27]. It is possible that once we have a way to identify and select those patients most likely to benefit from G‑POEM, the clinical success rate will increase further, and we will spare patients who are unlikely to respond. However, at this time, we cannot reliably predict the outcome of the procedure in advance.
Secondly, another reason for non-responsiveness to G‑POEM is possibly inadequate myotomy. Some studies used an intraoperative functional luminal imaging probe during G‑POEM to measure the distensibility or the cross-sectional area or diameter of the pyloric ring and tried to establish a criterium to predict the outcome of G‑POEM during the procedure [28,29,30]. However, all these studies are preliminary at this time and no firm conclusions have been made.
Thirdly, the single endoscopist in this study, QC, had performed more than 100 esophageal POEM procedures, a procedure similar to G‑POEM, before his first 16 G-POEM procedures at Emory University. Therefore, we cannot conclude at this time that the experience of an endoscopist has no effect on the outcome of G‑POEM for a less experienced submucosal endoscopist.
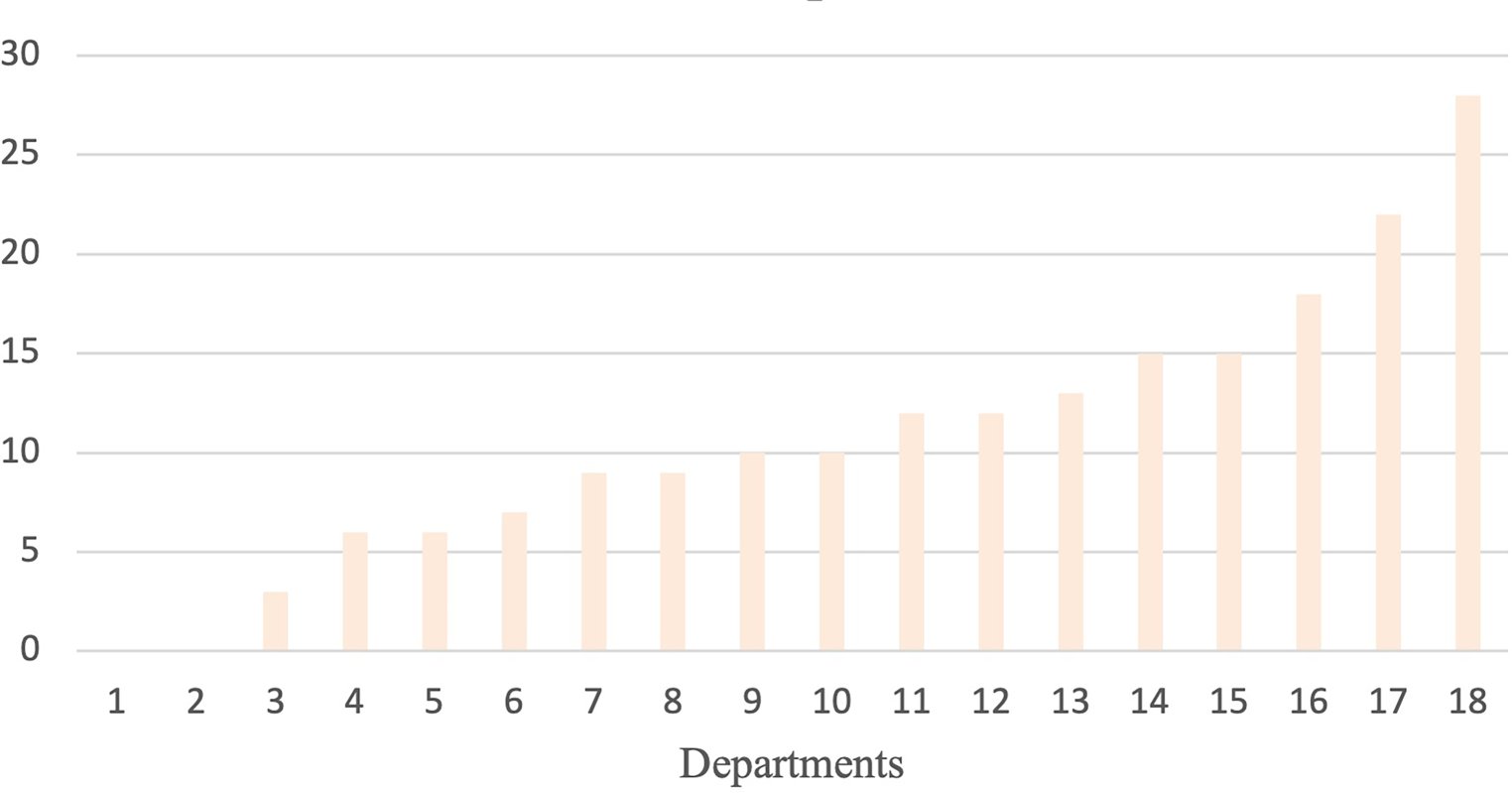
Although the clinical success rate did not change, the procedure time and length of hospital stay were significantly shorter in group B when compared to the earlier patients in group A. Procedure time dropped from an average of 49 min to 29 min. The group B patients underwent the procedure in an endoscopic center which had little to no experience in submucosal endoscopy prior to the study. Therefore, the procedure time for the group B patients might have been even shorter if the staff had been experienced. Furthermore, the length of hospitalization went down from an average of 2.5 days to 1.2 days. After our study on the first 16 patients in group A [12], we performed a study on same-day discharge after G‑POEM which showed that about 50% of patients could be discharged the same day after G‑POEM. However, to retain the comparison with group A, we kept all patients in group B for overnight observation and did not discharge any patients on the day of the procedure.
We acknowledge there are some limitations to this study: it is a single-center retrospective study with a small number of patients, the procedures were performed by the same endoscopist but not at the same institution, and the endoscopist already had POEM experience before performing G‑POEM on his initial 16 patients. Nevertheless, these data add important information to the literature by presenting short-term outcomes of G‑POEM in its early days and after multiple years of experience. It is an interesting finding that the efficiency has significantly improved in the past 8 years, with shorter procedure times and hospital stays, despite the clinical efficacy remaining stagnant at 80%. We feel that this finding emphasizes the fact that to further increase the clinical efficacy of G‑POEM, at least for an experienced endoscopist, more research is needed to optimize pre-procedure patient selection.





Comments (0)