
Remember me
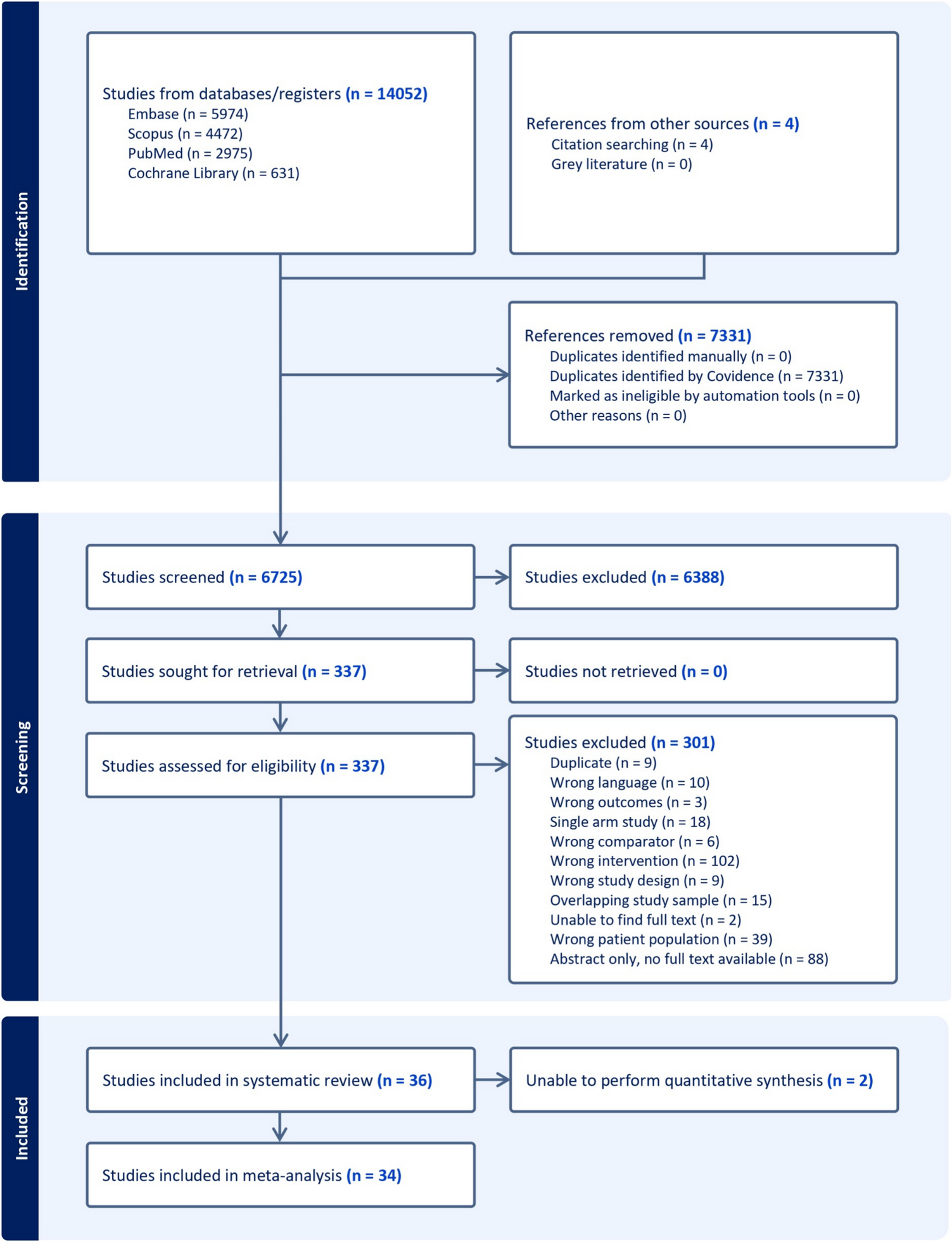
In this study, 191 cases of colorectal leiomyosarcoma were identified from 2000 – 2018 using the SEER database (Fig. 1).
Fig. 1
Flowchart for Colorectal Leiomyosarcoma
Demographic and Tumor CharacteristicsThe median age for the patients was found to be 64 years. The most common age groups were between the ages of 60–69 (23.0%) and 70–79 (23.0%). Females were the slight majority in this cohort with 54.5%, while 45.5% of the cases were male. In regard to race and ethnicity, the majority of patients were non-Hispanic white (78.0%), followed by non-Hispanic black (13.1%), non-Hispanic Asian or Pacific Islanders (7.3%), then non-Hispanic American Indian (0.5%).
When tumor grading was provided, most cases were poorly differentiated. Tumor sizes were known in 66.0% of cases. 7.9% of known cases were less than 2.0 cm, 26.2% were between 2.0 cm to 5.0 cm, and 65.9% were greater than 5.0 cm. The stage of the majority of cases were localized disease (45.5%) followed by regional (25.7%), then distant disease (15.7%) (Table 1). The tumor stage in 13.1% of cases was unknown. In 33.5% of the cases, the primary tumor site was the right colon (cecum to transverse colon), 35.6% in the left colon (splenic flexure to rectosigmoid junction), 23.6% in the rectum, and the primary site was unspecified in 5.2% cases. Lymph node status was known in 70.7% of cases. Of the statuses known, the majority of cases had positive lymph nodes (65.9%). While the site of distant metastases was unknown in the majority of cases, the most common site of metastasis was the liver (5.6%), followed by the lung (4.2%), and bone (1.1%) (Table 1).
Table 1 Demographic factors and tumor characteristics in colorectal leiomyosarcomaTreatment CharacteristicsOf the total cases, the majority of cases in this cohort underwent surgery only (74.9%) Only 2.1% of cases had chemotherapy only (any systemic therapy). No cases had radiation only. 3.1% of cases underwent combination therapy (surgery, radiation, and chemotherapy). 6.8% of cases did not undergo any treatment (Fig. 2).
Fig. 2
Pie chart describing treatment modalities
Overall and Disease-Specific Survival by TreatmentThe overall 5-year observed survival was 50.3% (95% C.I., 46.3—54.2) (Fig. 3a). The 5-year disease-specific survival (DSS) was 66.1% (95% C.I., 62.0—70.1) (Fig. 3b). The 1-year and 5-year survival with surgery only was 78.7% (95% C.I., 75.1—82.3) and 60.8% (95% C.I., 56.3—65.3), respectively. The survival analysis of chemotherapy only, radiation only, and other therapies not included in this analysis could not be performed due to a limited number of cases. There was a significant difference (p < 0.001) between surgery only, surgery + chemotherapy, no therapy, and other therapies (Fig. 4). Including patients with incomplete information did not change the results of the univariable or multivariable.
Fig. 3
(a) Overall survival of Colorectal Leiomyosarcoma (b) Disease-specific survival of Colorectal Leiomyosarcoma
Fig. 4
Overall Survival of Different Treatment Modalities. + Other includes Chemotherapy only, Surgery & Radiation, Chemotherapy & Radiation, Combination Therapy (Chemotherapy, Radiation, & Surgery)
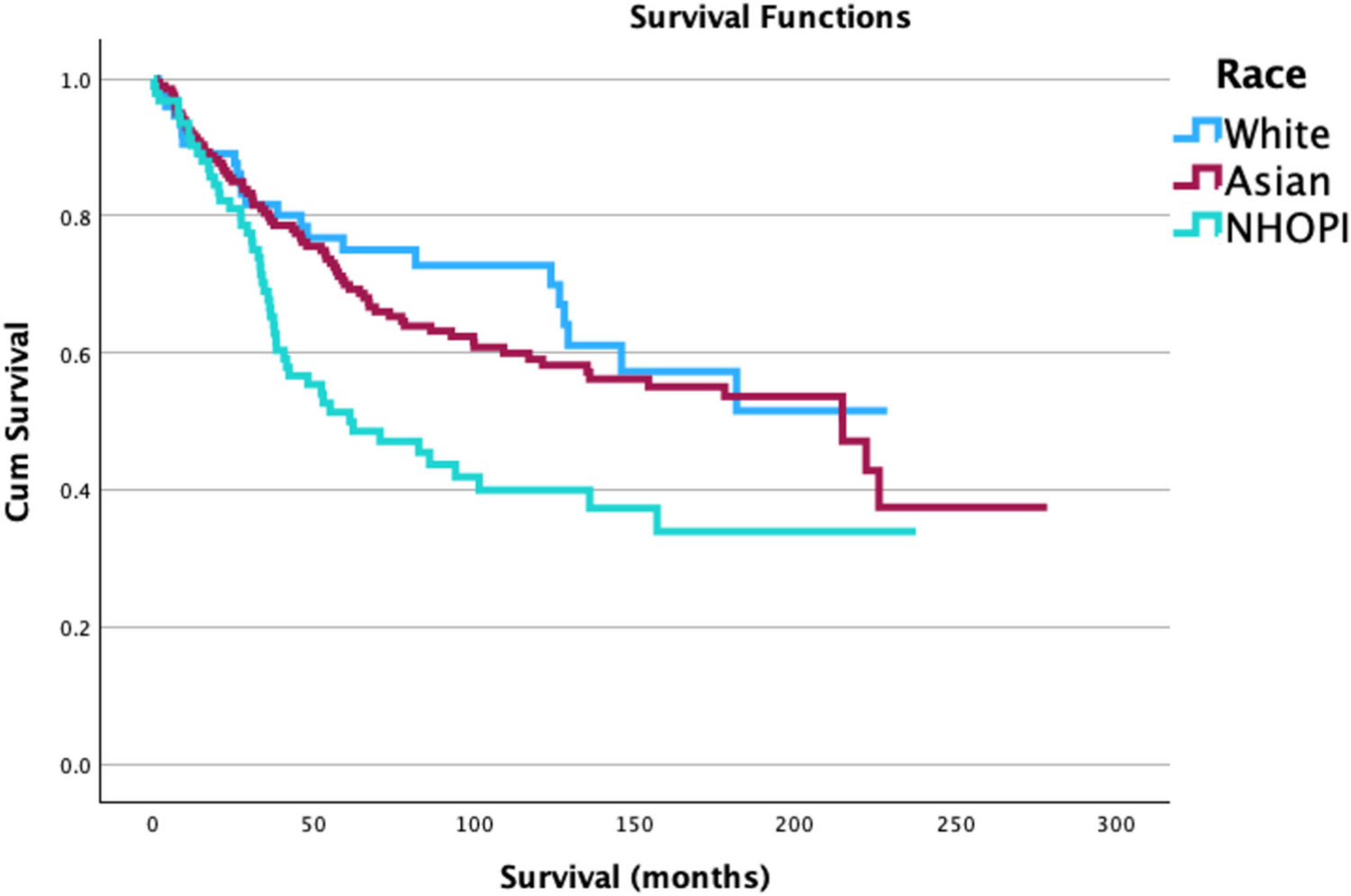
Overall Survival Analysis by Race and SexThere was no difference in percent survival rate amongst white, black, and other races (Supplemental Table 1). Race was not associated with survival rates (Fig. 5a).
Fig. 5
Survival of colorectal leiomyosarcoma by (a) race, (b) sex, (c) grade, (d) nodal status, (e) tumor size, and (f) tumor stage
There was no difference in percent survival rate between male and females (Supplemental Table 2) Sex was not a predictor for survival (Fig. 5b).
Overall Survival Analysis by Tumor CharacteristicsHigher grade was indicated as a negative predictor for survival (p < 0.001) (Fig. 5c). A positive nodal status was considered a negative prognostic factor for survival (p < 0.001) (Fig. 5d). Larger tumor size was indicated as a negative predictor for survival (p < 0.001) (Fig. 5e). A higher tumor stage was also a negative indicator of survival (p < 0.001) (Fig. 5f).
Univariable and Multivariable Analyses for Overall SurvivalUnivariable analysis indicated that increased age was a negative predictor (H.R. 1.036 (1.021—1.052), p < 0.001), that higher grade was a negative predictor (H.R. 1.645 (1.252—2.162), p < 0.001), and that a positive nodal status was a negative predictor (H.R. 2.25 (1.16–4.35), p = 0.016). Univariable analysis also revealed a tumor size of > 5 cm was a negative predictor for survival (H.R. 3.145 (1.707—5.793), p < 0.001) and that both regional stage (H.R. 2.02 (1.25–3.24), p = 0.004) and distant stage (H.R. 3.87 (2.31–6.47), p = < 0.001) were considered negative predictors. Univariate analysis revealed that undergoing surgery alone led to better outcomes (H.R. 0.34 (0.23–0.52) p < 0.001). Whether a patient underwent surgery and chemotherapy did not change the prognosis of survival in a patient (H.R. 1.72 (0.94–3.16), p = 0.079). Multivariable Cox proportional hazards analysis identified older age (H.R. 1.03 (1.01–1.05), p < 0.001), poorly differentiated grade III (H.R. 7.33 (2.35–22.91), p < 0.001), undifferentiated/anaplastic grade IV (H.R. 5.97 (2.04–17.50), p < 0.001), regional stage (H.R. 4.25 (2.20–8.21), p < 0.001), and distant stage (H.R. 6.07 (3.03–12.14), p < 0.001) as negative predictors for survival. Upon multivariate analysis it was determined that the treatment modalities of Surgery only & Surgery + Chemotherapy did not change prognosis of overall survival. Including patients with incomplete information did not change the results of the univariable or multivariable analyses (data not shown) (Table 2).
Table 2 Univariable & Multivariable analyses of independent factors influencing overall survival
Comments (0)