
Remember me

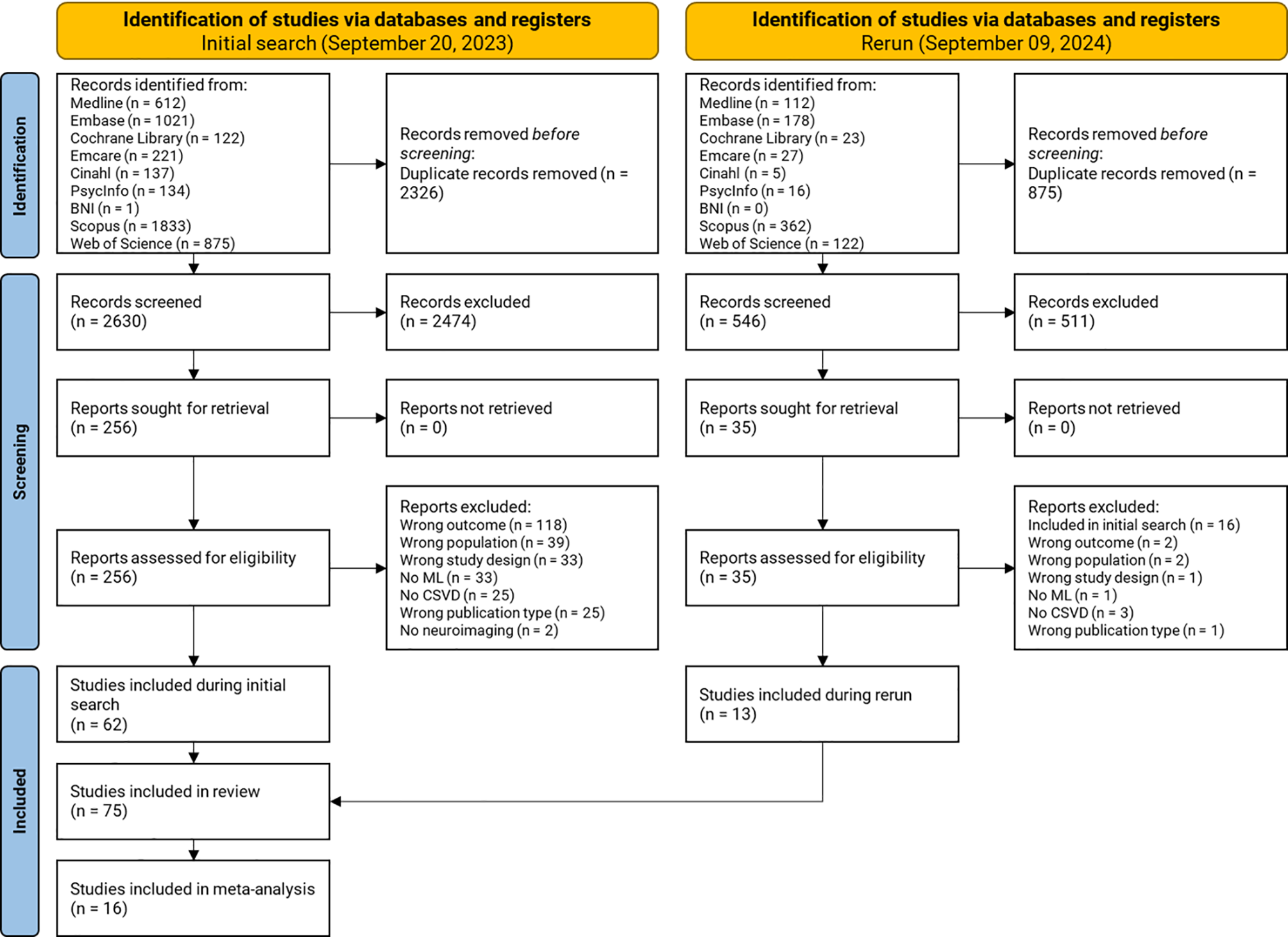

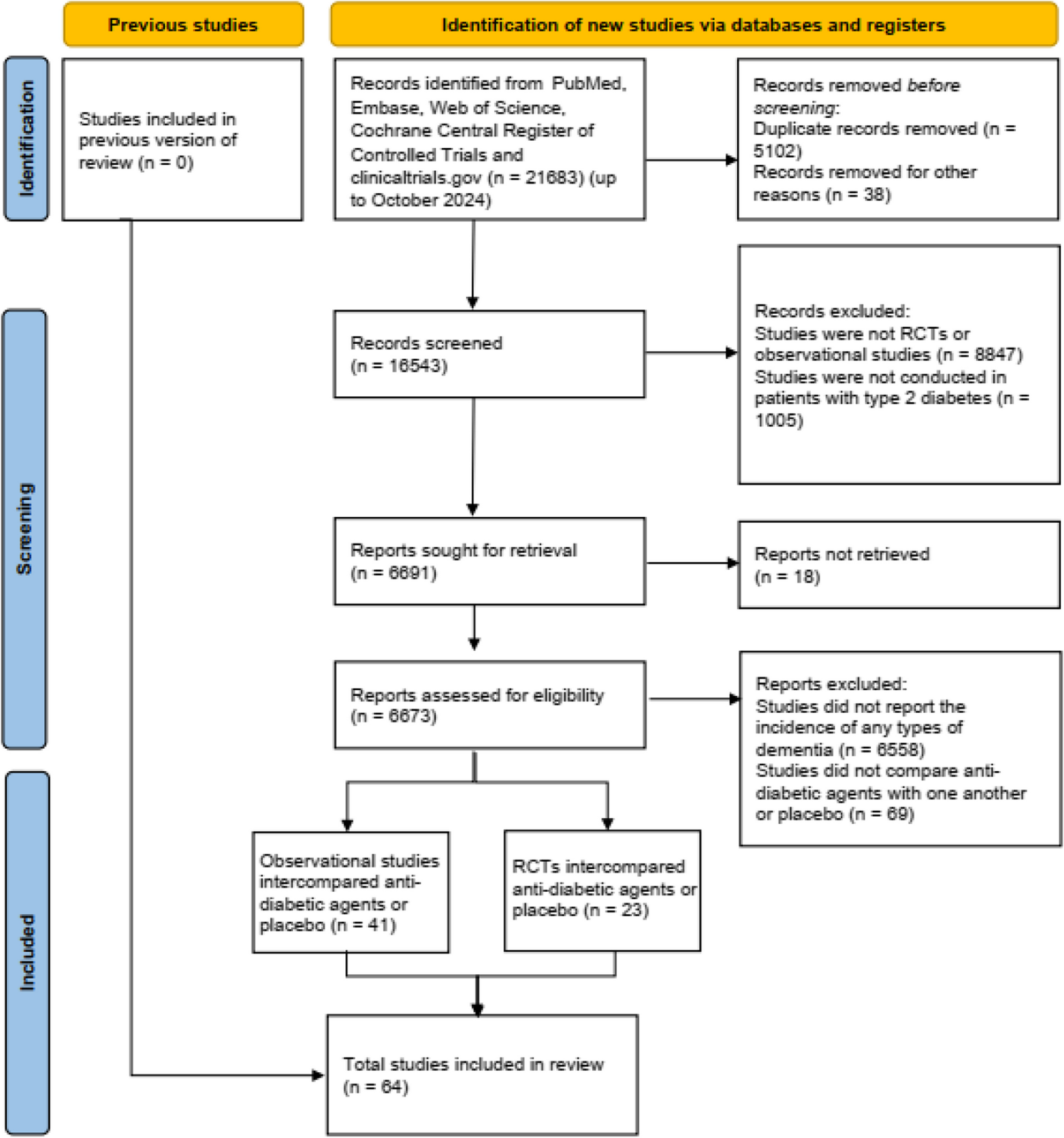

In total, there were 41 observational studies (including 34 cohort studies, 6 case-control studies and 1 cross-sectional studies) with 3,307,483 participants, and 23 RCTs with 155,443 participants included in the meta-analysis (Fig. 1). The anti-diabetic agents investigated in this research involve metformin, sulfonylureas, glinides, TZD, AGI, GKA, insulin, GLP-1RA, GLP-1/GIP receptor dual agonists, DPP-4i, and SGLT-2i. Baseline characteristics of included studies were summarized in Table S1.
Fig. 1
Flow diagram of this network meta-analysis
The quality assessments for observational studies and RCTs were implemented with Newcastle-Ottawa Scale (NOS) and Cochrane instruments respectively (Table S2, Table S3), which suggested generally low risks of bias in enrolled studies. For observational studies, the average score of NOS was 6.88 in cohort studies and 7.67 in case-control or cross-sectional studies, with 31 (75.6%) observational studies of high quality (score ≥ 7/9). For RCTs, there were 4 RCTs with uncertain bias of randomization sequence generation, 2 RCT with high risks for inadequate allocation concealment, and 4 RCTs with high risks for frequent missing outcome data. No RCT was with high risks of bias in adequate randomization sequence generation, or bias in selective outcome reporting, or bias in masking patients and caregivers, or bias in masking outcome assessors and adjudicators (Figure S1). The incoherence between direct and indirect evidence was evaluated by side-splitting charts, where no prominent incoherence was suggested (Table S4). Publication bias was assessed with funnel plots and Egger’s test. The funnel plots exhibited generally even distribution (Figure S2, Figure S3), and no significant publication bias was indicated by Egger’s test (Table S5).
Conventional meta-analysesFor observational studies, when compared with non-users, the risks of overall dementia were significantly lower in patients receiving metformin (OR = 0.92, 95%CI, 0.89 to 0.96, I2 = 92%), TZD (OR = 0.85, 95%CI, 0.80 to 0.90, I2 = 84%), DPP-4i (OR = 0.95, 95%CI, 0.91 to 0.99, I2 = 92%), SGLT-2i (OR = 0.75, 95%CI, 0.64 to 0.87, I2 = 97%) and GLP-1RA (OR = 0.75, 95%CI, 0.64 to 0.88, I2 = 93%). However, insulin (OR = 1.06, 95%CI, 1.01 to 1.11, I2 = 93%) and sulfonylureas (OR = 1.03, 95%CI, 1.00 to 1.16, I2 = 89%) treatment were associated with an increase in the risk of dementia when compared to non-users (Figure S4). Moreover, patients receiving SGLT-2i treatment were with significantly lower risks of Alzheimer’s disease (OR = 0.63, 95%CI, 0.56 to 0.70, I2 = 0%), when TZD treatment was associated with a reduced risk of Alzheimer’s disease (OR = 0.95, 95%CI, 0.94 to 0.97, I2 = 0%) and vascular dementia (OR = 0.71, 95%CI, 0.68 to 0.75, I2 = 0%). However, insulin treatment was associated with an increased Alzheimer’s disease risks (OR = 1.20, 95%CI, 1.18 to 1.22, I2 was not applicable), when compared with non-users (Figure S4).
In conventional meta-analysis of RCTs, no significant difference on the incidence of dementia were characterized in patients receiving TZD (RR = 0.99, 95%CI, 0.06 to 15.80, I2 was not applicable), DPP-4i (RR = 0.94, 95%CI, 0.53 to 1.68, I2 = 12%), SGLT-2i (RR = 1.55, 95%CI, 0.73 to 3.27, I2 = 0%), GLP-1RA (RR = 1.04, 95%CI, 0.55 to 1.97, I2 = 0%) (Figure S5) when compared with non-users. Similarly, no significant associations were observed among anti-diabetic agent treatment and other dementia subtypes including Alzheimer’s disease, vascular dementia, frontotemporal dementia, and dementia with Lewy bodies (Figure S5).
We also conducted meta-regression analyses to address the influence of potentially associated factors on study results. For observational studies, age was found negatively associated with the risks of dementia (β = −0.016, 95% CI, −0.028, −0.003, p = 0.014), suggesting that patients who were older would gain more prominent benefits in dementia risks reduction with anti-diabetic treatment. While for RCTs, no baseline characteristic was found to be associated with the risks of dementia in patients with T2D. Further details on meta-regression analyses were summarized in Table S6 .
Network meta-analysesNetwork meta-analyses of observational studiesThe network diagrams of observational studies are exhibited in Fig. 2 and Figure S6 Compared with non-users, SGLT-2i (OR = 0.56, 95%CI, 0.45 to 0.69), GLP-1RA (OR = 0.58, 95%CI, 0.46 to 0.73), TZD (OR = 0.68, 95%CI, 0.57 to 0.81) and metformin (OR = 0.89, 95%CI, 0.80 to 0.99) treatments were associated with the reduced risk of dementia in patients with T2D. Moreover, the risk of dementia was significantly lower in patient receiving SGLT-2i treatment when compared to those using metformin (OR = 0.56, 95%CI, 0.45 to 0.69), DPP-4i (OR = 0.65, 95%CI, 0.52 to 0.80), GKA (OR = 0.53, 95%CI, 0.29 to 0.99) and AGI (OR = 0.62, 95%CI, 0.39 to 0.97). Besides, patients with GLP-1RA treatment also presented lower risks of dementia compared with metformin (OR = 0.65, 95%CI, 0.51 to 0.83) and DPP-4i (OR = 0.67, 95%CI, 0.52 to 0.86). However, compared with placebo, insulin (OR = 0.85, 95%CI, 0.67 to 1.08) and sulfonylureas (OR = 0.97, 95%CI, 0.84 to 1.12) did not increase the risk of dementia in patients with T2D (Table 1).
Fig. 2
Network plots for observational studies (evaluating the risks of dementia). *Abbreviations: PBO, placebo; MET, metformin; TZD, thiazolidinediones; SU, sulfonylureas; AGI, α-glucosidase inhibitor; DPP-4i, dipeptidyl peptidse-4 inhibitor; SGLT-2i, sodium-glucose cotransporter-2 inhibitor; GLP-1RA, glucagon-like peptide-1 receptor agonist; GKA, glucokinase activator.
Table 1 League charts of observational studies. League charts of observational studies intercomparing the risks of dementia among different anti-diabetic agents and placeboFurthermore, SGLT-2i (OR = 0.43, 95%CI, 0.30 to 0.62), GLP-1RA (OR = 0.54, 95%CI, 0.30 to 0.96) and DPP-4i (OR = 0.73, 95%CI, 0.57 to 0.93) treatments were associated with significantly reduced risk of Alzheimer’s disease when compared with non-users. Other than life intervention, the risk of Alzheimer’s disease was reduced in patients treated with SGLT-2i when compared with those receiving metformin (OR = 0.46, 95%CI, 0.31 to 0.68), TZD (OR = 0.52, 95%CI, 0.34 to 0.79), DPP-4i (OR = 0.59, 95%CI, 0.45 to 0.78), insulin (OR = 0.28, 95%CI, 0.15 to 0.53) and sulfonylureas (OR = 0.46, 95%CI, 0.31 to 0.66) (Table 2).
Table 2 League charts of observational studies. League charts of observational studies intercomparing the risks of Alzheimer’s disease among different anti-diabetic agents and placeboAs for vascular dementia, SGLT-2i (OR = 0.42, 95%CI, 0.22 to 0.80) and TZD (OR = 0.52, 95%CI, 0.36 to 0.75) were associated with a lower risk of vascular dementia compared with non-users. Meanwhile, SGLT-2i conferred greater risk reduction in vascular dementia compared with metformin (OR = 0.32, 95%CI, 0.15 to 0.68), DPP-4i (OR = 0.48, 95%CI, 0.27 to 0.85) and sulfonylureas (OR = 0.32, 95%CI, 0.16 to 0.65) (Table 3).
Table 3 League charts of observational studies. League charts of observational studies intercomparing the risks of Alzheimer’s disease among different anti-diabetic agents and placeboIn terms of SUCRA evaluation for the dementia, the rank order was SGLT-2i (SUCRA: 94.5, mean rank: 1.5) > GLP-1RA (SUCRA: 92.1, mean rank: 1.8) > TZD (SUCRA: 80.5, mean rank: 3.0) > DPP-4i (SUCRA: 57.4, mean rank: 5.3) > metformin (SUCRA: 54.0, mean rank: 5.6) > AGI (SUCRA: 47.3, mean rank: 6.3) > GKA (SUCRA: 31.1, mean rank: 7.9) > sulfonylureas (SUCRA: 25.7, mean rank: 8.4) > glinides (SUCRA: 24.1, mean rank: 8.6) > insulin (SUCRA: 11.3, mean rank: 9.9), which indicated SGLT-2i and GLP-1RA might serve as the optimal treatments in reducing the risk of dementia in patients with T2D. And regarding benefits in reducing the risk of Alzheimer’s disease, the rank was: SGLT-2i (SUCRA: 94.9, mean rank: 1.4) > GLP-1RA (SUCRA: 81.3, mean rank: 2.5) > DPP-4i (SUCRA: 66.7, mean rank: 3.7) > AGI (SUCRA: 56.7, mean rank: 4.5) > TZD (SUCRA: 55.3, mean rank: 4.6) > metformin (SUCRA: 34.9, mean rank: 6.2) > sulfonylureas (SUCRA: 33.9, mean rank: 6.3) > insulin (SUCRA: 3.9, mean rank: 8.7). As for vascular dementia, the rank was GLP-1RA (SUCRA: 84.3, mean rank: 1.9) > SGLT-2i (SUCRA: 83.4, mean rank: 2.0) > TZD (SUCRA: 75.6, mean rank: 2.5) > DPP-4i (SUCRA: 47.8, mean rank: 4.1) > metformin (SUCRA: 11.8, mean rank: 6.3) > sulfonylureas (SUCRA: 10.8, mean rank: 6.4) (Figs. 3, 4 and 5; Table 4).
Fig. 3
SUCRA evaluations of the network meta-analysis for observational studies. SUCRA evaluations of the network meta-analysis for observational studies (anti-diabetic agents and the risks of dementia)
Fig. 4
SUCRA evaluations of the network meta-analysis for observational studies (anti-diabetic agents and the risks of Alzheimer’s disease)
Fig. 5
SUCRA evaluations of the network meta-analysis for observational studies (anti-diabetic agents and the risks of vascular dementia). Abbreviations: TZD, thiazolidinediones; AGI, α-glucosidase inhibitor; DPP-4i, dipeptidyl peptidse-4 inhibitor; SGLT-2i, sodium-glucose cotransporter-2 inhibitor; GLP-1RA, glucagon-like peptide-1 receptor agonist; GKA, glucokinase activator.
Table 4 Results of SUCRA probability evaluation for observational studiesNetwork meta-analyses of RCTsThe network diagrams of RCTs are shown in Fig. 6 and Figure S7 According to the results, compared with placebo, no significantly altered dementia risks were observed in patients receiving DPP-4i (RR = 1.19, 95%CI, 0.61 to 2.32), SGLT-2i (RR = 0.45, 95%CI, 0.67 to 3.12), GLP-1RA (RR = 1.08, 95%CI, 0.57 to 2.05), TZD (RR = 0.73, 95%CI, 0.09 to 32.74), or sulfonylurea (RR = 1.75, 95%CI, 0.66 to 4.63). With respect to the risks of Alzheimer’s disease, vascular dementia, and dementia with Lewy bodies, no significant associations were observed when intercomparing all anti-diabetic agents and placebo as well. More detailed results were summarized in Figure S8 and Table S6-7.
Fig. 6
Network plots for randomized controlled trials (evaluating the risks of dementia)
Comments (0)