ROP is a biphasic retinal disease, starting with a retinal ischemia due to the downregulation of VEGF and Insulin-Like Growth Factor 1 (IGF-1) and the retinal vascularization arrest ending in overproduction of VEGF from ischemic retina and neovascularization induction. So, anti-VEGF agents and retinal ablation therapy reduce the burden of vitreous VEGF, preventing extreme neovascularizations and abnormal vessel formations [9]. These therapeutic interventions are recommended in type 1 ROPs and aggressive ROP (A-ROP) to prevent more advanced complications of ROP, such as retinal detachments [10].
Anti-VEGF agents have been widely used and approved in treating various retinal diseases such as diabetic retinopathy (DR), Age-Related macular degeneration (AMD), and retinal vein occlusion (RVO) for a long time. It has been suggested that these agents may induce long-term changes in retinal compartments besides the therapeutic targets. The increase in optic disk cup size is one of the long-term side effects related to these agents in DR [11]. On the other hand, a study showed an increase in papillary VD after anti-VEGF therapy in RVO cases [12]. However, Some reports have shown that the macular VD does not change after treatment with anti-VEGFs in DR or AMD [13, 14, 15]. On the other hand, a study demonstrated a decrease in macular VD after treatment with such agents in DR [16].
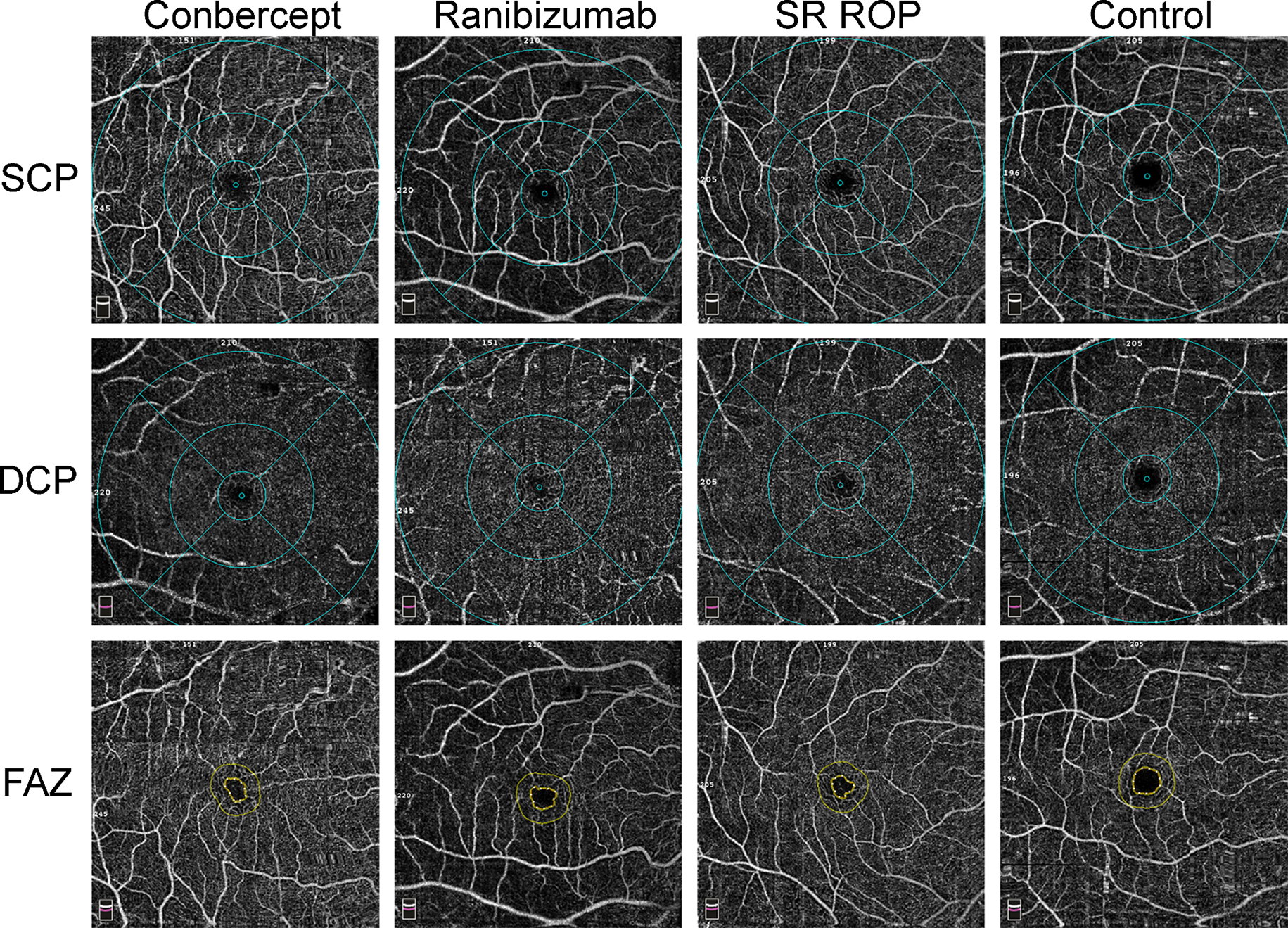
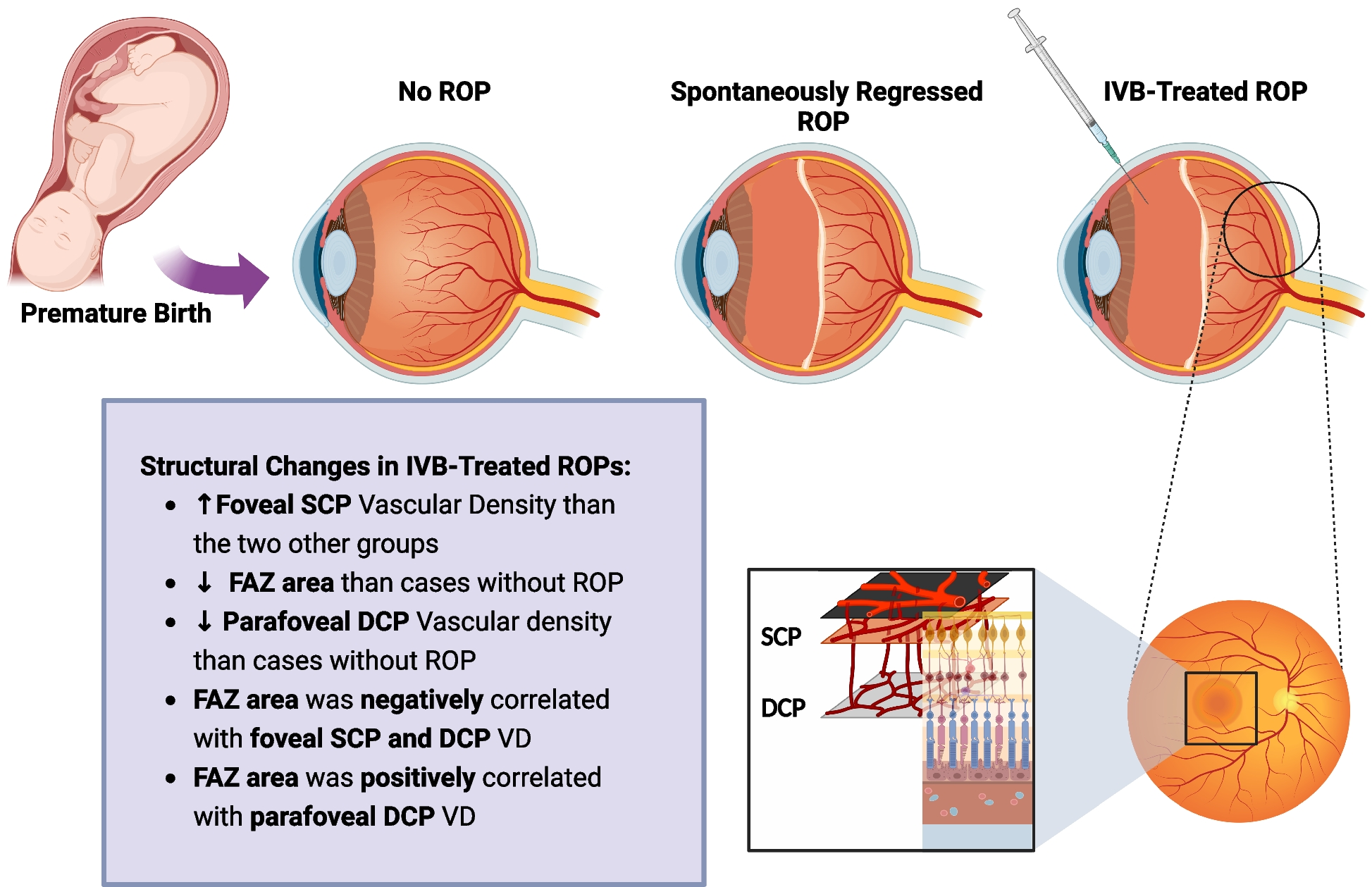
In recent years, with the increased use of anti-VEGF agents in treating ROP cases, attention has been drawn to studying the short and long-term effects of these medications on the retina in pediatrics. Our retrospective cohort study aimed to evaluate the macular microvascular status in three groups of preterm children: 1. Preterm children without ROP, 2. Preterm children with spontaneously regressed ROP, and 3. ROP cases treated with IVB. Our results show a significantly higher VD in the foveal SCP in the IVB-treated ROPs compared to two other groups (28.56% vs. 22.90 and 23.10% in SR and PT groups, respectively). However, parafoveal DCP had a lower VD in the IVB group compared to the PT group (48.55 vs. 53.45%).
Besides, the FAZ area was significantly smaller in the IVB group than in the preterm cases without ROP (0.113 mm2 vs. 0.219). Furthermore, the higher the foveal vascular density, the smaller the FAZ area.
The prevalence of microvascular abnormalities was significantly higher in the IVB group than in the SR group. However, it was mainly due to the more advanced cases in the IVB group. Based on our findings, microvascular abnormalities were associated with more advanced ROPs and worse BCVA.
A recently published meta-analysis demonstrated a smaller FAZ area in preterm children than in term cases. It declared that preterm cases without ROP had a larger FAZ area than those with ROP. Also, IVB and laser-treated ROPs had smaller FAZ than SR cases, which is coherent with our findings. The foveal SCP VD was significantly higher in IVB-treated ROPs than in preterm cases without ROP, and it was also higher than in SR cases, which is confirmed by our findings [17]. Although this study tried to contribute the smaller FAZ in IVB and laser-treated ROPs to the more advanced forms of ROP and higher levels of VEGF, based on our findings, the FAZ area was smaller in the IVB group compared to the PT group and not compared to the SR cases. Also, the comparison between various ROP zones revealed a significant difference in the FAZ area. Although this meta-analysis is a beneficial source in studying the microvascular status of ROP cases, it should be considered that only two studies out of 11 included studies have evaluated the IVB-treated ROPs, and the total number of IVB-treated cases was 127.
Chen et al. reported a smaller FAZ area and higher foveal VD in anti-VEGF treated ROP cases compared to the normal healthy children and correlated the higher foveal superficial plexus VD to the worse BCVA [18]. Although this study was coherent with our study regarding the FAZ area and foveal VD changes, we failed to show any correlation between the BCVA and these variables. In addition, the BCVA in their study was worse than ours regarding the anti-VEGF treated cases (0.10 vs. 0.045). This difference may be due to the more advanced staging of the cases; all of their cases were stage 3 in zones 1 and 2.
Another study on 25 anti-VEGF-treated ROPs compared to 22 laser-treated ROPs showed a significantly larger FAZ area and higher parafoveal VD (deep and superficial) in the first group. However, the stagings were similar between the two groups. Their results regarding the parafoveal superficial plexus VD and FAZ area were comparable with ours (50.86% and 0.14 mm2, respectively). However, their reported value for the parafoveal deep plexus VD was higher than ours (54.15% vs. 49.5%) [19]. The difference between the laser and anti-VEGF treated cases regarding the FAZ area and parafoveal VD is notable because patients with similar stagings but different treatments showed different FAZ area and parafoveal VD measurements in both of these findings.
We believe two possible hypotheses may justify these differences regarding the FAZ area. The first concerns the role of pigment epithelial-derived factor (PEDF) in FAZ area development and its relationship to PRP and anti-VEGF factors. The literature findings are controversial regarding the role and condition of the PEDF in ROP cases; however, PEDF concentrations are believed to decrease in ROP cases [20]. On the other hand, some studies demonstrated that anti-VEGF agents could increase the PEDF concentration and decrease the VEGF/PEDF ratio to inhibit angiogenesis [21]. Concerning the highly determining role of PEDF concentration and expression in FAZ area development in the embryonic and neonatal period [22], the smaller FAZ area in IVB-treated cases than the preterm cases, without a significant difference with the SR cases may be due to other systemic conditions of the ROP cases, which affected the PEDF and VEGF balance in the eye even before ROP screening. Based on our results, the SR group demonstrated an intermediate amount of FAZ area between the IVB-treated and PT cases. The IVB-treated cases have had more advanced stages of ROP, which shows they have had a more stressful systemic condition, such as hypoxia, low birth weight, and sepsis. Because foveal blood circulation develops earlier than peripheral areas, these cases with smaller FAZ areas may have experienced more predisposing conditions to systemic or ophthalmic ischemia, leading to the deregulation of PEDF expression even in the embryonic period. Nevertheless, more molecular studies on the effect of PRP and anti-VEGF agents on the VEGF/PEDF ratio in ROP cases may reveal a new era in this field.
The second hypothesis concerns the correlation of the parafoveal deep plexus VD and FAZ area. As mentioned, the lower parafoveal deep plexus VD was associated with a smaller FAZ area. This finding may be related to possible ischemia induced by lower parafoveal deep plexus VD, leading to reduced PEDF and increased VEGF in the foveal region, inducing more development and migration of vessels to the center of the macula.
Regarding the higher prevalence of macular microaneurysms and telangiectasia in IVB-treated cases, the IVB could not be recognized as the causative agent, and the presence of these microvascular abnormalities before the treatment should be considered. Also, the more advanced stages in the IVB-treated cases should not be denied. Newer retinal imaging techniques with handheld Swept-Source OCTA would be beneficial in detecting the exact relationship between these findings [23].
Although our study is one of the few studies evaluating and comparing the macular microvascular condition of anti-VEGF-treated ROP cases to the spontaneously regressed ROPs and preterm cases without ROP yet, the lack of variables regarding the systemic condition and inclusion of both eyes of the patients in the study are limitations of our study. Besides, our sample size was mediocre, so more extensive studies with larger sample sizes, including PRP and anti-VEGF-treated cases and comparing them with SR and preterm cases, eliminating all the possible confounding variables' impact, would help strengthen the available evidence in this field and improve the therapeutic guidelines.




Comments (0)