
Remember me



A 39-year-old woman with a long-standing history of high myopia presented with visual field constriction, reported by the patient to have been present for 20 years. She had well-controlled diabetes mellitus, hyperlipidemia, and chronic migraine. She denied any history of trauma and no significant surgical or social history. She reported that peripheral visual field constriction had begun 20 years ago and had worsened over the past two months. She also reported mild to moderate morning headaches, pulsatile tinnitus, and intermittent periocular pain. Her body mass index was 30.14 kg/m2, and blood pressure was normal. Neurological examination revealed normal cranial nerve function.
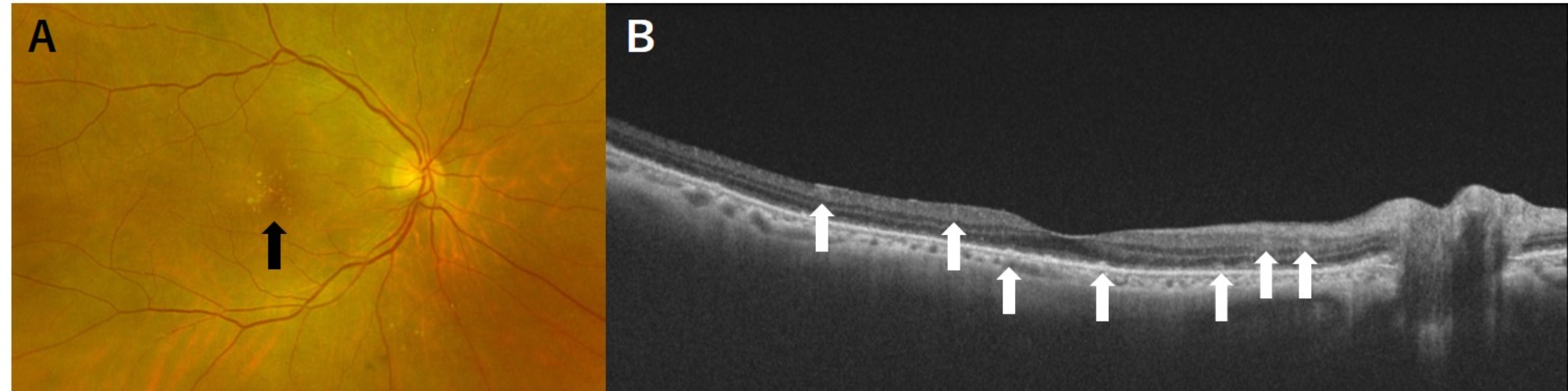
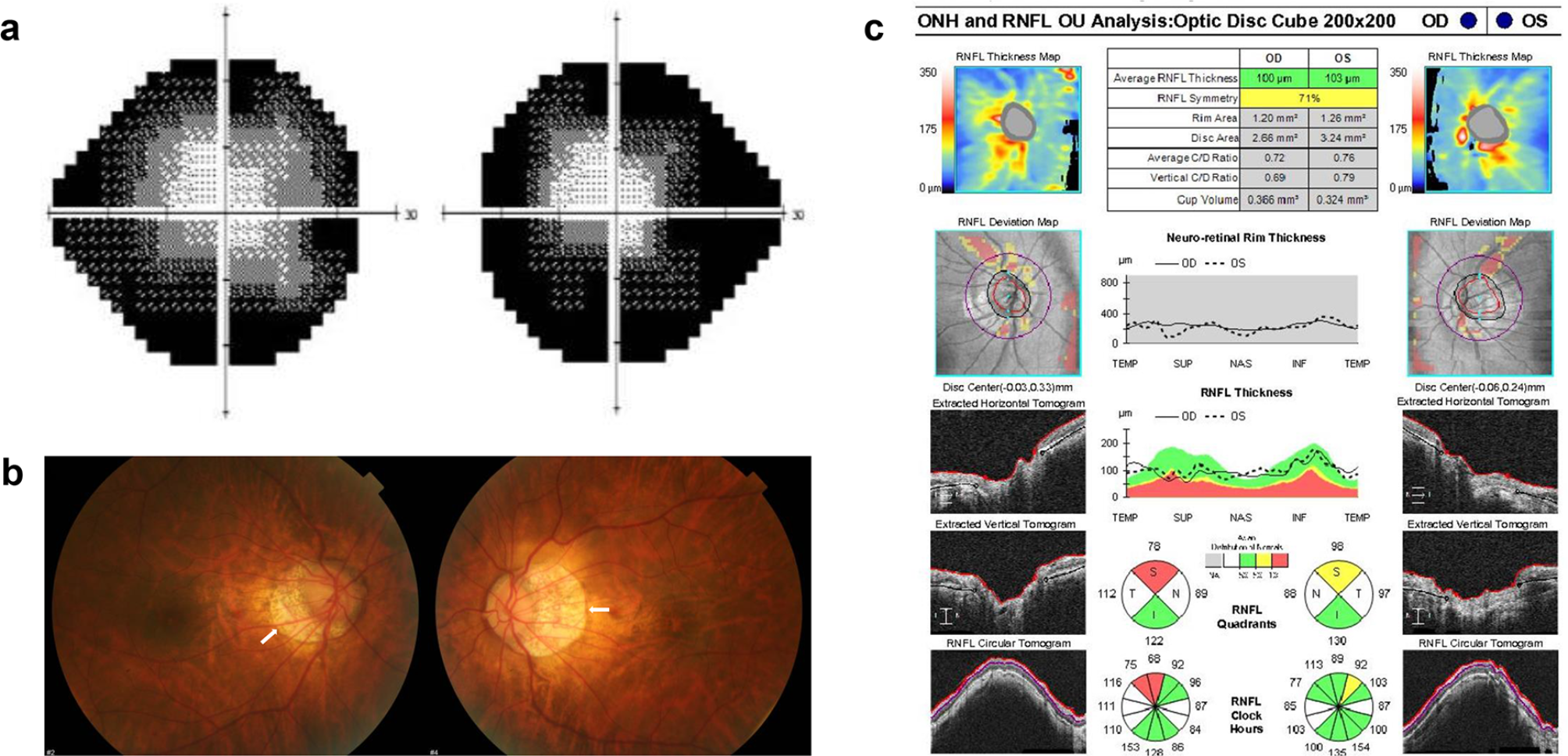
On ocular examination, the best-corrected visual acuity was 20/30 in the right eye with − 9.0 Diopter Sphere, and − 3.0 Diopter Cylinder at 180º axis, and 20/50 in the left eye with − 10.0 Diopter Sphere, -3.5 Diopter Cylinder at 10 º axis. The intraocular pressure measured by air pulsation was elevated in both eyes: 23 mmHg in the right and 25 mmHg in the left. Visual field examination revealed a constricted visual field in both eyes (Fig. 1a). Fundus photography revealed the characteristic features of high myopia, including a tilted disc and peripapillary atrophy (Fig. 1b). Disc swelling was not identifiable in any eye. The average thickness of the retinal nerve fiber layers in both eyes on optical coherence tomography (Cirrus HD-OCT; Carl Zeiss Meditec, Dublin, CA, USA) was within the normal range (Fig. 1c). Macular structures and electroretinography results were normal.
Fig. 1
Ocular examination results on the initial visit. a Visual field test reveals bilateral concentric visual field contraction. b Fundus photography demonstrates features of high myopia. The peripapillary gamma zone is marked with a white arrow. c Cirrus high-definition optical coherence tomography shows nearly normal thickness of peripapillary retinal nerve fiber layers
Laboratory tests revealed normal complete blood counts, electrolyte levels, liver function, kidney function, and serum angiotensin-converting enzyme levels. Antinuclear, antineutrophil cytoplasmic, anticardiolipin, anti-aquaporin 4, and paraneoplastic antibodies were negative.
Orbital magnetic resonance imaging (MRI) showed no significant abnormalities, including intensity changes, compression, or kinking of the optic nerve. Brain MRI and magnetic resonance venography also revealed no structural defects, hydrocephalus, meningeal enhancement, empty sella, or venous sinus thrombosis.
A cerebrospinal fluid (CSF) study revealed an elevated opening pressure of 27.2 cmH₂O, confirming increased intracranial pressure (IICP). The CSF cell count and biochemistry were normal, and no malignant cells were detected on cytology.
Considering her symptoms and confirmation of elevated CSF opening pressure, treatment with 250 mg of acetazolamide tablets three times daily was initiated for IIH symptom control. After one month, her headache and tinnitus gradually improved. Six months later, her visual field had markedly improved (Fig. 2a), and her visual acuity was 20/25 in both eyes. IOP was 19 mmHg in the right eye and 21 mmHg in the left eye. The tinnitus and periocular pain resolved, and the headache was relieved.
Fig. 2
Ocular examination results six months after treatment initiation. a Visual field test reveals marked recovery of visual field. b Fundus photography demonstrates severe bilateral peripapillary atrophy, showing no significant change compared to previous images
Comments (0)