Demographics
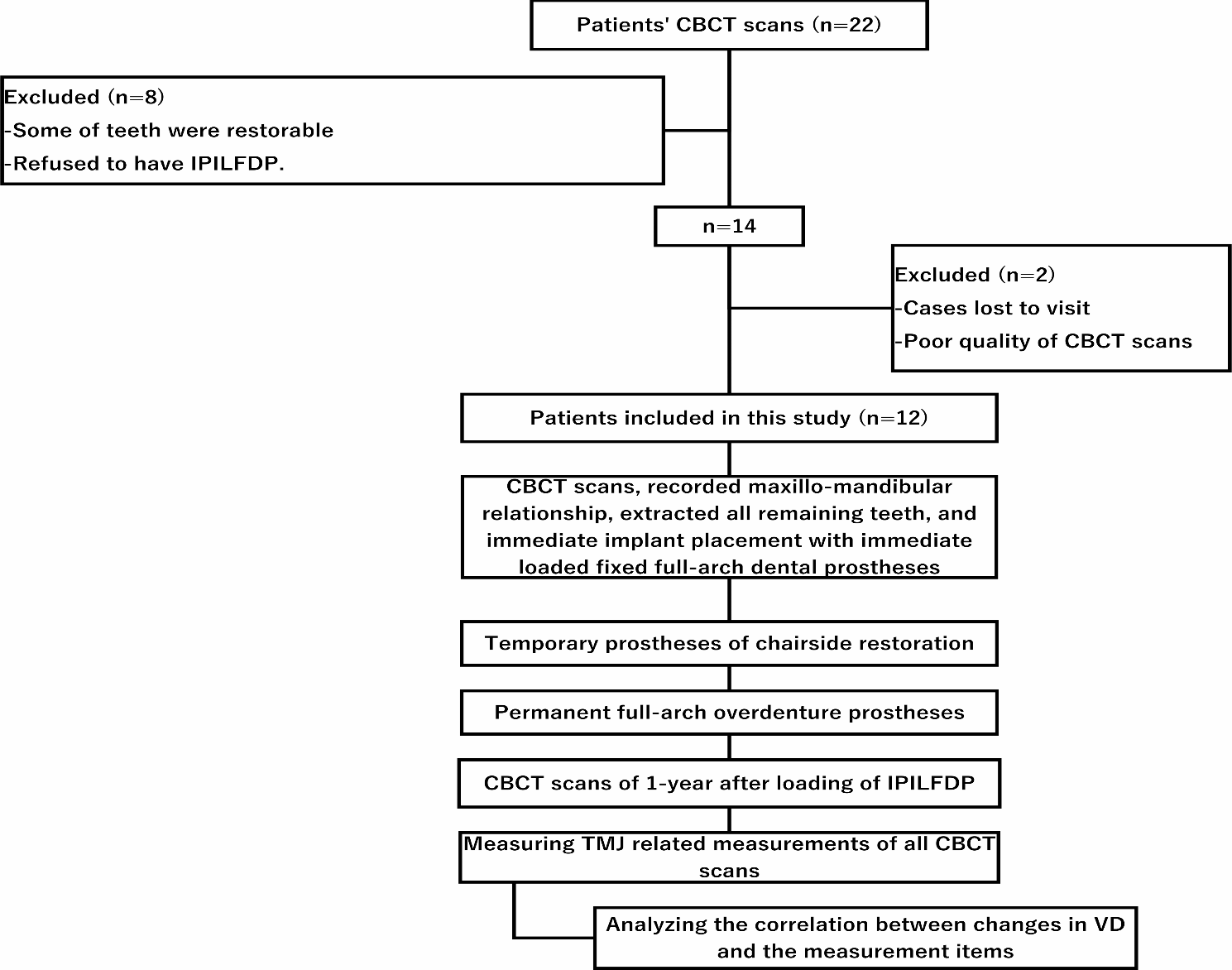
Maxillary edentulous patients who visited the University dental school clinic from March 2021 to October 2022 for implant-supported prosthesis treatment and underwent CBCT were evaluated. A total of 48 patients were collected. The edentulous arches were classified using the Cawood and Howell classification. Of these patients, eleven were excluded because their alveolar bone classification was categorized as level III. Nine patients were excluded due to inadequate CBCT images that precluded the virtual design of zygomatic implants. Ultimately, 28 participants were included in the study, comprising 12 males and 16 females, with an average age of 63.8 ± 12.6 years. The 28 edentulous maxillae were divided into 56 hemi-maxillae, with 39 of the 56 edentulous posterior residual ridges classified as Class IV and the remaining 17 as Class V/VI. In total, 112 implants were virtually planned.
BIC of zygomatic implantsBIC of the anterior zygomatic implant
The apex points of the anterior ZIs were at A0, A1, A2, and A3. The total BIC (tBIC) and the zygomatic BIC (zBIC) of implants decreased significantly from A3 to A0 (P < 0.01, Table 1) while the alveolar BIC (aBIC) showed no significant change (P = 0.769). The average zBIC at A3, A2, A1, and A0 was 18.3 ± 3.9 mm, 13.4 ± 3.7 mm, 7.4 ± 2.8 mm, and 4.2 ± 1.7 mm respectively.
In the Class IV subgroup, tBIC and zBIC decreased from A3 to A0, with a significant difference observed among ZIs at all apex points (P < 0.01), However, no significant difference was found in aBIC among implants at any apex points (P = 0.849).
In the Class V/VI subgroups, tBIC and zBIC also decreased from A3 to A0. A significant difference in zBIC was noted among implants at all apex points (P < 0.01), while no significant difference was observed in tBIC between implants at A3 and A2 (P = 0.217), or between those at A1 and A0 (P = 0.132). The tBIC of implants at A3 and A2 was significantly higher than that of implants at A1 and A0 (P < 0.05). No significant difference in aBIC was found among implants at any apex points (P = 0.939).
For implants at the four apex points of the upper zygoma, no significant difference in tBIC, zBIC, or aBIC was detected between the two subgroups (P > 0.05).
Table 1 Total BIC, zygomatic BIC and alveolar BIC in the anterior zygomatic implants (mm)BIC of the posterior zygomatic implant
The apex points of the posterior implants comprised eight locations: B0, B1, B2, and B3 at the middle zygoma, and C0, C1, C2, and C3 at the lower zygoma. Within the B series, the highest zBIC and tBIC were recorded at the B2 point (16.3 ± 5.3 mm; 22.1 ± 7.5 mm), while the C series showed the highest values at the C1 point (13.8 ± 5.0 mm; 19.5 ± 5.5 mm) as indicated in Table 2. The B2 point demonstrated the highest zBIC and tBIC among all eight apex sites, with a significant difference from the other points. No significant difference in zBIC and tBIC were observed among the B1, B3, C1, and C2 points (zBIC at B3: 13.4 ± 4.8 mm, at B1: 13.5 ± 5.5 mm, at C1: 13.8 ± 5.0 mm, at C2: 12.3 ± 5.8 mm), though these were significantly higher than those at the B0, C0, and C3 points (zBIC at B0: 8.9 ± 4.9 mm, at C0: 10.9 ± 4.1 mm, at C3: 8.5 ± 4.5 mm). Across all apex points, aBIC did not show significant variation (P > 0.05) (Table 2).
In the Class IV and Class V/VI subgroups, the highest BIC was noted at the B2 point in the middle zygoma and at the C1 point in the lower zygoma. For Class IV subgroup, zBIC and tBIC at the B2 point were significantly higher compared to other apex points. Between the C1 and B1 apex points, no significant difference in zBIC and tBIC was detected. In the Class V/VI subgroup, zBIC and tBIC did not significantly differ between the B2 and B1 points, but a significant difference was found between the B2 point and other points, excluding B1 (Table 2).
No significant difference was found in aBIC and tBIC of implants at the same apex points between Class IV and V/VI subgroups.
Table 2 Total BIC, zygomatic BIC and alveolar BIC in the posterior zygomatic implants (mm)Relationship between zygomatic implants and the Infratemporal Fossa (Table
3)Anterior zygomatic implants and infratemporal fossa
For the anterior zygomatic implants, only one of the 56 implants (1.8%) at the A3 point intruded into the infratemporal fossa. The depth of the intrusion was 1.2 mm. No other anterior implants showed entry into the fossa. There was no significant difference in the rate of ZI intrusion among the four apex points (A series points) (P = 0.390).
The single implant that intruded into the infratemporal fossa was from the subgroup of class IV, although there was no significant difference in the rate of anterior ZI intrusion between the two subgroups.
Posterior zygomatic implants and infratemporal fossa
For the B series apex points (mid-zygoma), no implant intrusion into the infratemporal fossa was observed at B0. However, intrusion rates at B1, B2, and B3 were 1.8%, 42.9%, and 92.9%, respectively, with the average depth and length of intrusion into the infratemporal fossa increasing progressively. The average intrusion depth was 2.4 mm, 2.2 ± 1.0 mm, and 3.9 ± 1.6 mm at B1, B2, and B3 respectively. Significant differences in intrusion rates were noted between B3 and B0, and B2 and B0, but not between B1 and B0.
For the C series apex points (lower zygoma), varying rates of ZI intrusion into the infratemporal fossa were recorded across the four sites. From C0 to C3, the intrusion rate, depth and length of ZI exposure in the infratemporal fossa increased (Table 3). At the C3 apex point, all implants intruded into the infratemporal fossa, with an average intrusion depth of 7.8 ± 2.6 mm. Significant differences in intrusion rates were present among all C series sites.
In Class IV subgroup, no ZI intrusion into infratemporal fossa occurred at B0 and B1 site, while 35.9% of the ZI at B2 site and 89.7% of the ZI at B3 site showed intrusion, with intrusion depth of 2.4 ± 1.0 mm (B2) and 3.9 ± 1.7 mm (B3). For the C series apex points, 15.4% of ZI at C0, 56.4% of ZI at C1 site, and over 90% of ZI at C2 and C3 sites entered the infratemporal fossa (Table 3), with intrusion depths increasing from C0 to C3.
Within the Class V/VI subgroup, there was no ZI intrusion into the infratemporal fossa at the B0 site, and only one ZI at the B1 site (5.9%) penetrated the infratemporal fossa with an intrusion depth of 2.4 mm. In contrast, 58.8% of ZIs at the B2 site and all ZIs at the B3 site (100%) intruded into the infratemporal fossa (Table 3). Regarding the C series sites, 23.5% of ZIs at the C0 site, 64.7% of ZIs at the C1 site, and over 90% of ZIs at both the C2 and C3 sites entered the infratemporal fossa (Table 3). Although the exact values for ZI intrusion rate, as well as the average depth and length of intrusion, were higher in the Class V/VI subgroup compared to Class IVsubgroup, there was no statistically significant difference in the rate, depth, or length of ZI intrusion at any of the middle and lower zygoma apex sites between the two subgroups (P > 0.05).
Table 3 Intrusion rate and depth and length of quad zygomatic implant intruded into infratemporal fossaThe risk of orbital cavity penetration
No orbital cavity penetration was detected in all the cases at all apex points. The distance between the anterior ZI and the orbital cavity was shown in Table 4. The average distance between the anterior ZI and the orbit was 2.5 ± 1.0 mm, 3.2 ± 1.0 mm, 3.8 ± 1.0 mm, and 4.3 ± 0.9 mm at A3, A2, A1, and A0 apex points respectively. There was significant difference in ZI-orbital distance among the four apex groups (P < 0.001). No significant difference in ZI-orbital distance was found between the Class IV and Class V/VI subgroups at all the A series points. Three anterior ZI at A3 point showed less than 1 mm distance from the orbital cavity.
Table 4 The closest distance between the anterior zygomatic implant and the orbital cavity at different apex points (mm) 



Comments (0)