
Remember me






This prospective cohort study leverages the UKB database, which was recruited between 2006 and 2010, over 500,000 participants aged 37–73 years from 22 assessment centers across the UK contributed to this resource [13]. The database underwent regular updates, including multiple follow-up surveys. Ethical approval was granted by the North West Multicenter Research Ethics Committee (REC reference for UKB 11/NW/0382), and all participants provided written informed consent. The complete study protocol of the UKB database is available at https://www.ukbiobank.ac.uk/media/gnkeyh2q/study-rationale.pdf.
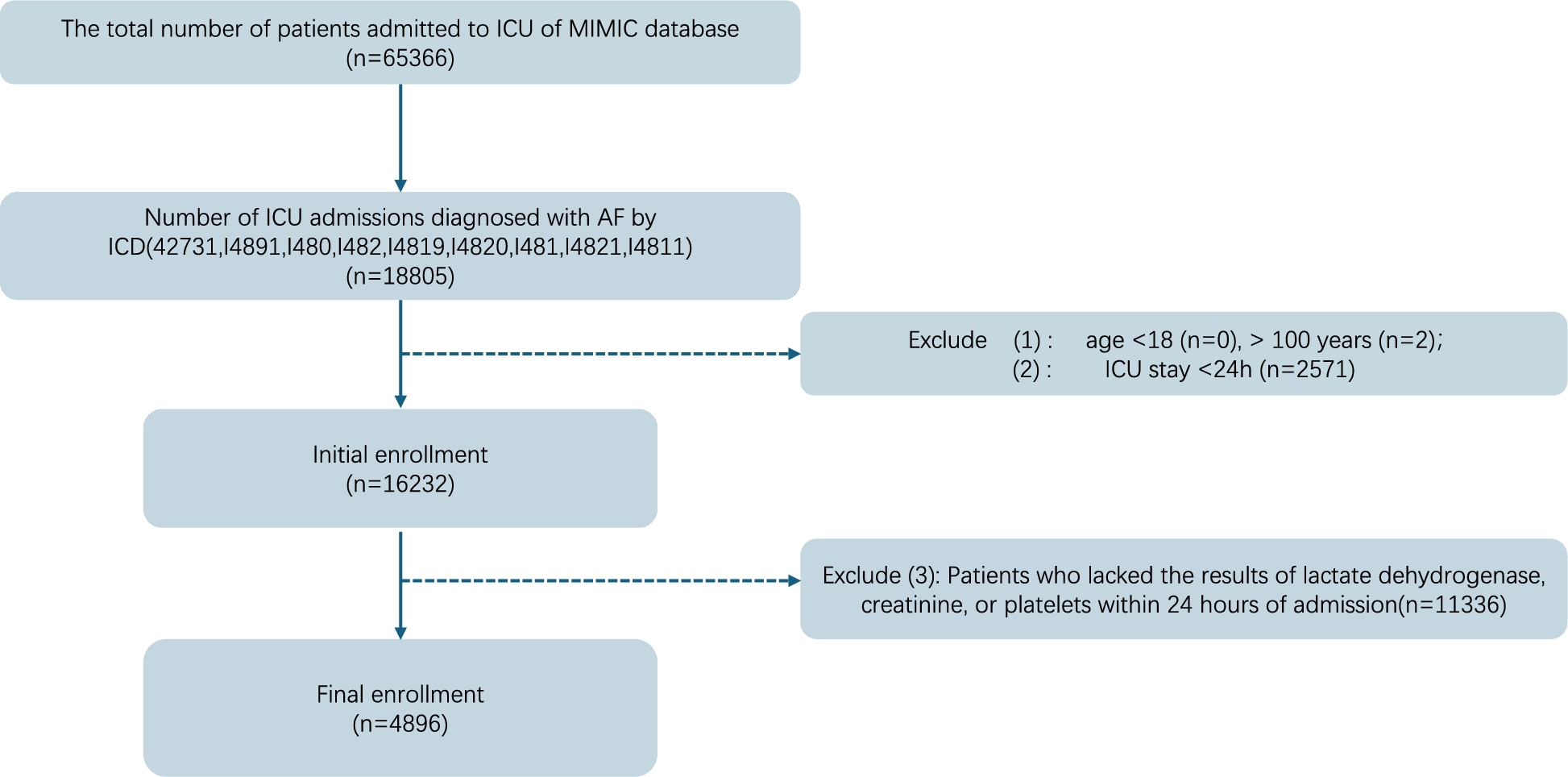
In our study, a total of 502,367 UK adults underwent initial screening. Exclusions were made for individuals lacking data on loneliness (n = 35,705), those with a baseline arrhythmia diagnosis (n = 14,384), and those without information on PRS for AF (n = 11,222), resulting in 441,056 participants for our analyses (see Fig. 1). Additional details on the participant selection process can be found in Supplementary Method 1.
Fig. 1
Study flowcharts. Abbreviations: PRS, polygenic risk scores; UK, United kingdom.
Assessment of exposureTo be consistent with previous studies conducted in UKB cohorts [15,16,17], the evaluation of loneliness focused on the subjective perception of loneliness and the willingness to confide in others [8, 17]. The methods used in this study to assess loneliness and social isolation have beenvalidated among UKB database-based studies, dating back as far as a article discussing the relationship between loneliness and social isolation and heart attacks and strokes, which was the first time such methods were used to assess loneliness and social isolation in the paper, flatly analogous to the Revised UCLA published back in 2004 [14, 15]. Loneliness was assessed by two questions from questionnaires: “Do you often feel lonely?” (1 point for the response of “yes” and 0 point for “no”) and “How often are you able to confide in someone close to you?” (1 point for the response of “never or almost never” and 0 point for the response of “once every few months”, “once a month”, “once a week”, “2–4 times a week”, or “almost daily”). The loneliness score was calculated by summing the scores from both questions, resulting in a range of 0–2 points. Participants were categorized into two groups based on their loneliness score: the no-loneliness group (0 or 1 point) and the loneliness group (2 points).
Social isolation was evaluated by a method which focused on objective social connections, including frequency of social interactions or engagement in social activities [18]. Social isolation was evaluated through responses to three questions on questionnaires: (1) “How often do you visit friends or family or have them visit you?” (1 point for the response of “once a month”, “once every few months”, “never or almost never”, or “no friends or family outside the household” and 0 point for the response of “once a week”, “2–4 times a week”, and “Almost daily”); (2) “Which of the following leisure or social activities do you engage in once a week or more often? You may select more than one of them: sports club or gym, pub or social club, religious group, adult education class, or other group activities” (1 point for the response of “none of above” and 0 point for the response of one of activities mentioned above); and (3) “Including yourself, how many people live in your household? Include those who usually live in the house such as students living away from home during term time, and partners in the armed forces or in professions such as pilots” (1 point for the response of “0” and 0 point for other numbers higher than 0). The social isolation score was derived by summing up the points from the three questions, resulting in a range of 0 to 3. Participants were categorized into three groups based on their social isolation score: least isolated group (0 points), moderately isolated group (1 point), and most isolated group (2 or 3 points). The field ID of the questions above is presented in Supplementary Table 1.
Assessment of outcomeAF was the primary outcome of this study. The diagnosis of AF was established through a comprehensive review of hospital admission data and cause-of-death registry records. This included hospital admission data from the Hospital Episode Statistics for England (up to October 31, 2022), Scottish Morbidity Record data for Scotland (up to July 31, 2021), and Patient Episode Database for Wales (up to February 28, 2018). Additionally, the study incorporated death cause registry records from the National Health Service (NHS) Information Centre (England and Wales, up to November 30, 2022) and the NHS Central Register, National Records of Scotland (Scotland, up to November 30, 2022). Confirmation of AF occurred when there was a medical diagnosis evident in the hospital admission data or when AF was specifically listed as a cause of death in the death register. Diagnostic data collection adhered to the International Classification of Diseases, Tenth Revision (ICD-10), with the code for AF designated as ICD I48 [19]. No AF would be confirmed unless there was a medical diagnosis evident in the hospital admission data or when AF was specifically listed as a cause of death in the death register. Information obtained by the remaining modalities that participants may have AF was not taken into account. In addition, the time at which the patient developed AF and whether or not the patient had developed AF prior to inclusion in the study was also specified by the manner in which it was defined above.
Assessment of covariatesCovariates for this study were collected at baseline. Covariates included age, sex, race/ethnicity, body mass index (BMI), assessment center, Townsend derived index, educational level, current smoking, alcohol consumption, physical activity, healthy sleep score, self-reported medical conditions (history of hypertension, diabetes, high cholesterol, ischemic heart disease, heart valve diseases, cardiomyopathy, stroke, hyperthyroidism, cancer, and statins use), and glucose or lipid metabolism measures from laboratory tests on blood samples.
The Townsend derived index is a measure of material deprivation within a population. The measure incorporates four variables: (1) unemployment (as a percentage of those aged 16 and over who are economically active); (2) non-car ownership (as a percentage of all households); (3) non-home ownership (as a percentage of all households); and (4) household overcrowding. These variables can be measured for the population of a given area (based on the participant’s postcode), higher scores indicate a higher degree of deprivation [20]. Physical activity was measured by the metabolic equivalent task (MET) [16]. Healthy sleep score calculated based on sleep traits including insomnia, sleep duration, chronotype, daytime sleepiness, and snoring [range 0–5, the higher the better] [19].
Grades of genetic risk (low, moderate, and high genetic risk) were defined according to the tertiles of the PRS to AF. The calculation of the PRS to AF from the UKB database has been previously described [19]. Specific information on covariates in the cohort is presented in Supplementary Method 2 and the field ID of the questions above in the UKB is presented in Supplementary Table 1.
Statistical analysesBaseline variables with continuous variables are expressed as mean ± standard error or median (interquartile range), and categorical variables are expressed as frequency (percentage). Statistical differences for continuous variables were analyzed using the two-sample t-test or ANOVA test, and categorical variables were analyzed using the χ2 test.
For missing data, we estimated the median for variables with missingness rate < 5%, and treated missing data as a separate category labeled “unknown” for variables with missingness rate ≥ 5%. Detailed information on the covariates with a missingness rate ≥ 5% is presented in Supplementary Table 2.
The Cox proportional hazards model was used to calculate hazard ratios (HRs) and 95% confidence intervals (CIs) for the incidence of AF with multivariate adjustment. Model 1 adjusted for age, sex, and race/ethnicity; Model 2 further adjusted for BMI, assessment center, Townsend deprived index, college/university degree, currently smoking, alcohol consumption, physical activity, and healthy sleep score. Model 3 was further adjusted for hypertension, diabetes mellitus, high cholesterol, ischemic heart disease, heart valve disease, cardiomyopathy, stroke, hyperthyroidism, cancer, statin, and PRS to AF. In addition, the associations of loneliness with AF were further explored in participants with different heart valve disease statuses and levels of genetic susceptibility to AF (low, moderate, and high genetic risk).
In supplementary analyses, the cumulative risk of incident AF among different groups is presented in Kaplan–Meier curves with a log-rank test. In addition, we explored the association of loneliness with AF in study participants with different levels of social isolation. Furthermore, we performed subgroup analyses of the association between loneliness and AF risk. Subgroup analyses were performed by stratifying by age (< 65 years old or ≥ 65 years old), sex (male or female), race/ethnicity (white or others), obesity (BMI ≥ 30 kg/m2; yes or no), Townsend derived index (< 50% or ≥ 50%), etc. In addition to the entire population, we repeated the primary analysis among participants with excluded cardiomyopathy and among participants with excluded hyperthyroidism, respectively, to eliminate the effect of known etiologies. Finally, we excluded those diagnosed with AF within the first year of follow-up to mitigate the potential impact of reverse causality. Also, we further used the Fine–Gray sub-distribution hazard model to account for the potential impact of mortality as a competing event.
All analyses were performed using R version 4·3·0 (R Foundation for Statistical Computing, Vienna, Austria), and statistical significance was set at P < 0·05 for two-sided testing.
Role of the funding sourceThis project was funded by CAMS Innovation Fund for Medical Sciences (No. 2021-I2M-1–008). In this study, the funding was mainly user for getting access to the UKB database. Besides, we declare that the funding had no role in the writing of this manuscript or the decision to submit it for publication.
Comments (0)