
Remember me


A scenario was developed in collaboration with subject matter experts from the fire brigade, the Belgian Armed Forces, and the Brussels Intercommunal Transport Company (BITC). In this scenario, a nerve agent is released in a busy subway station beneath a populous winter fairground. This scenario is predicated on the 1995 Tokyo sarin attack, during which the nerve agent sarin was disseminated in multiple subway stations by a terrorist cult [9].
Two aerosol-generating devices are strategically positioned proximate to subway exits. Upon the arrival of the subway train, these devices are activated synchronously to release sarin gas. Concurrently, passengers disembark from the train and traverse through the aerosolized toxic clouds to exit the station, while others embark on the train. The impacted individuals manifest a spectrum of symptoms, from minor ocular and respiratory irritation to acute neurological manifestations such as confusion, agitation and seizures. Incapacitated victims prevent the doors of the train from closing, causing a cessation of train movement on that side of the station.
Immediate communication is established with the national 112 emergency dispatch center (HC112) and the BITC, leading to an immediate cessation of subway line operation and the remote opening of turnstiles for expedited egress. The emergent clinical manifestations among multiple individuals precipitate a state of panic, culminating in a secondary, more chaotic, evacuation phase during which additional traumatic injuries occur.
HC112 identifies the surge in call volume and symptomatology indicative of a chemical incident. In response, multiple deployments of ambulance units and MMTs are initiated, along with the HAZMAT component of the fire brigade. The standard ambulance units are staffed with two basic EMTs, while MMTs consist of an emergency physician and an emergency nurse. Given the suspected chemical mass casualty incident, the specialized CBRNe MMT is dispatched alongside HAZMAT teams.
Upon arrival, the response teams delineate the impacted area into hot, warm, and cold zones, corresponding to varying levels of threat and contamination. HAZMAT teams equipped with Personal Protective Equipment (PPE) commence search and rescue operations within the subway station, simultaneously establishing a medical response chain that includes decontamination procedures. Evacuated individuals are directed to a CCP where triage is initially performed by a physician and a nurse, both equipped with PPE. Triage categories are reassessed after each medical intervention or before each transport.
Post-CCP triage and decontamination, the victims are divided into two cohorts. Ambulatory and mildly affected individuals are conveyed via chartered buses to outpatient medical facilities or even discharged to their residences, their condition allowing. Non-ambulatory individuals are integrated into the medical response chain and subsequently transported to a Forward Medical Post (FMP). At the FMP, victims either undergo stabilizing medical intervention prior to hospital transport or are directly conveyed to designated hospitals with in-transit medical care. Upon hospital arrival, definitive treatment for both chemical and traumatic injuries is administered, marking the ending of the simulated scenario for this victim. The simulation ends when all victims either have received final treatment or are deceased.
Computer SimulatorThe SIMEDIS Simulator constitutes a discrete-event simulation model, utilizing the Julia programming language and predicated on the functionalities offered by the SimJulia package [10, 11]. Central to the simulation environment is the victim model, which records each victim’s spatiotemporal location and evolving health state throughout the entire care continuum. Upon initiation, the simulator loads a pre-defined scenario that encompasses an event timeline, a list of victims, resource inventories, and a set of scenario-specific parameters which are included in appendix 1.
The simulator is designed to implement the Belgian Medical Contingency Plan for disasters, incorporating key elements such as an incident site, a CCP, an optional FMP, and hospitals. Victims are transported between these locations with transport durations being dependent upon the mode of transport and calibrated for each simulated scenario.
Victims flow through the simulation pipeline, starting at the incident site and ending at designated medical facilities. The simulator monitors both the geographical location and the health state of each victim. The latter is governed by a computational victim model elaborated upon in subsequent sections of this publication. Medical interventions can be performed at multiple locations —namely, the incident site, the CCP, the FMP, and within ambulance units—and serve to improve the victims’ health states, consequently extending their potential survival duration, either temporarily or indefinitely.
To account for uncertainty in the timelines, stochastic variability is integrated into S&R, treatment and transport durations. This probabilistic approach serves to better approximate real-world uncertainties and contingencies, thereby augmenting the robustness and generalizability of the simulation results [12].
Sarin dispersion.
Sarin was chosen for its historical precedence in both human and animal studies, as well as its occurrence in accidental and intentional exposures. Its relatively low persistence and ease of synthesis make it a plausible choice for non-state actors [13]. Additionally, sarin can be rapidly identified using field testing kits, although real-world scenarios may experience delays in agent identification, potentially leading to secondary contamination and overestimations of the agent’s physicochemical properties [14, 15]. For the purposes of this simulation, we assumed no secondary contamination among healthcare providers and a sufficiency of resources for FMP treatment and antidote administration.
To rigorously evaluate the disaster response chain, case-mix heterogeneity is required. While scenarios predominated by either unsalvageable victims or those with trivial intoxication levels are plausible in real-world situations, such extremes are not the focus of this research question. The quantity of sarin gas released in the subway station was determined with this in mind.
For the quantification of sarin exposure within the subway environment, an analytical Gaussian Puff dispersion Model (GPM) was constructed to yield a credible yet computationally tractable exposure dose [16]. In parallel, an experimentally validated Computational Fluid Dynamics model of the subway station was developed to explore the airflow patterns, particularly the impact of a moving train on local air circulation. The resulting model shows that the windspeed effects of a stopped train on sarin dispersal at the chosen point are limited. The GPM parameters correspond to an estimated 654 g of Sarin being released using an improvised dispersal device at speeds of 2 g per second. This dispersal rate and quantity are well within limits posited by experts of the US Department of Homeland Security and used in a similar study [17]. A more detailed description of the dispersion model and the concentrations achieved over time can be found in Appendix 2.
Passenger Flow and Injury AssignmentVictims are instantiated at the incident site and navigate their egress from the subway station. To model the evacuation, we use a social force model as implemented in the Vadere open-source framework for pedestrian dynamics [18]. The actual station architecture is replicated to construct a realistic evacuation model, including the dimensions of obstructions such as the train and staircases.
Two distinct evacuation waves are modeled to simulate varied behavioral responses. The initial wave represents an orderly egress consistent with standard operational procedures, while the second wave consists of a disordered evacuation characterized by panic-induced stampeding and consequent crush injuries and asphyxia. For each individual, a time-concentration integral is computed based on their specific evacuation trajectory and exposed time, as well as the chemical cloud generated by the dispersion model. This allows for the calculation of the individualized dose for each victim. During the second, disordered, evacuation wave, victims are subject to crush-induced traumatic injuries. A compendium of such injuries and their respective frequencies was constructed, drawing on retrospective analyses of stampedes found in the literature. These injuries span a spectrum from superficial lacerations and contusions to severe conditions such as traumatic asphyxia and vertebral fractures [19, 20]. Victims who can self-evacuate, do so on their own accord and will have left the station after 3 min. Victims who cannot self-evacuate due to their health state are evacuated by the HAZMAT (S&R) team. This evacuation process is described in more detail in appendix 2.
The mechanical force exerted on each individual during the evacuation process is derived from the amount of overlap between the circles of influence of the evacuees in the social force model [21]. This total sustained force is used as a proxy to hierarchically assign the corresponding injuries.
Victim ModelFor the purposes of this simulation research, a victim health state model was developed, building upon prior foundational models in the field [22,23,24]. This newly conceptualized health state, henceforth referred to as the Simedis score (SS), incorporates parameters and categories that are consistent with validated trauma scoring systems [25, 26]. The parameter categories incorporated into the SS are as follows: Glasgow Coma Scale (GCS), oxygen saturation, respiratory frequency, heart rate, and systolic blood pressure. These metrics were selected based on their clinical relevance and utility in trauma care:
Glasgow Coma Scale (GCS): Provides a comprehensive evaluation of a patient’s level of consciousness.
Heart Rate: Serves as an indicator of both the patient’s level of intoxication and their hemodynamic stability.
Systolic Blood Pressure: Functions as a surrogate measure for organ perfusion and, by extension, organ function.
Respiratory Rate: Acts as a diagnostic marker for both the level of dyspnea and metabolic acidosis.
Oxygen Saturation: Included due to its frequent and straightforward measurement in prehospital trauma care, as well as its utility in differentiating between levels of injury severity. For this parameter, categorization was informed by a comprehensive literature review [27].
Through the incorporation of these clinically significant parameters, the SS aims to provide a nuanced and comprehensive assessment of a victim’s health state and it’s need for urgent life-saving interventions. The components and their scoring values used in the SS are visualized in Table 1.
Table 1 Overview of the components used in the Simedis score, their categories and corresponding valuesTraumatic InjuriesAnalysis of previously developed traumatic victim models revealed that clinical progression of categorical victim health scores of untreated victims can be modeled using a sigmoid curve. While others have been proposed, we chose to use a generalized Gompertz curve because of its simplicity and history of applications in modeling growth and mortality [28,29,30,31]. Using a set of trauma victims from earlier experiments and data available in the literature, we fitted the parameters to the generalized Gompertz curve based on the victim’s Injury Severity Score (ISS) and age [32]. We refer to appendix 2 for a more detailed explanation describing the assumptions and equations used.
Chemical InjuriesIn parallel to the traumatic evolution, we modeled the effects of chemical injury. For this we assume 7 discrete chemical injury profiles, corresponding to increasing levels of intoxication. These range from very mild (injury profile 1) to lethal (injury profile 6), as well as the absence of intoxication (injury profile 0). These injury profiles are assigned corresponding to a victim’s exposure and are based on military models adapted for civilian purposes [33, 34]. Vital signs and symptoms were added to these victims based on expert opinion in conjunction with existing animal and human experimental data as well as pharmacokinetic/pharmacodynamic models available in the literature [35, 36].
TriageAs mentioned previously, triage is performed by a triage physician or nurse wearing adequate protection. Triage is based on the NATO triage system for chemical injuries and the SALT triage method for traumatic injuries [37, 38]. The exact implementation is described in appendix 2. For immobile victims, triage is assumed to take 30 s, and 5 s for walking victims. A victim receives both a chemical and a traumatic triage category, and the highest (most serious) triage category of either determines the final triage category. This triage category determines decontamination, treatment and evacuation order. In the case of identical triage categories between victims, the SS is used as a tie breaker.
Decontamination and AMSDecontamination is implemented as a time-delay in parallel lanes and includes disrobing, dry padding with absorbent materials and then re-robing. The decontamination and AMS times are based on internal experiments performed at a tertiary hospital in Brussels, which are comparable with times reported in the literature [39, 40]. Mobile victims self-decontaminate, and immobile victims get decontaminated by the firefighters.
An AMS team is present to stabilize severely injured and contaminated victims. Their location depends on the strategy. They identify the victim with the highest triage category, remove it from their waiting queue and administer a limited stabilizing treatment. This treatment consists of antidotes, as well as anticonvulsive and respiratory support if necessary. After their intervention the victim returns to the transport or decontamination queue it was originally in, at the highest priority position.
TreatmentTreatment effects can be modeled as improvements over time that slow the deterioration or improve the victim’s SS. This improvement can be either temporary or permanent. The act of treatment has a duration based on the triage category and ISS, and the effect of the treatment is based on the provider’s skill level. The duration and effect of the treatment is described in appendix 2. Treatment takes effect instantly, therefore contact of a victim with a treatment provider instantly prolongs the survival time.
Variable ParametersPretriagePreliminary triage (pretriage) is a limited triage that is performed in the subway station to determine the order of Search and Rescue. Victims receive either a yellow (low priority) or a red (high priority) disk from the HAZMAT team members. Pretriage differs from the actual triage which takes place at the CCP, is performed by doctors and nurses, and determines treatment and evacuation order. If pretriage is set to true, the order by which victims arrive at the CCP is determined by the SS at time of contact with the pretriage team. In the case of a tie, a First-In-First-out principle is used. When no pretriage is carried out the victim arrival list is randomized.
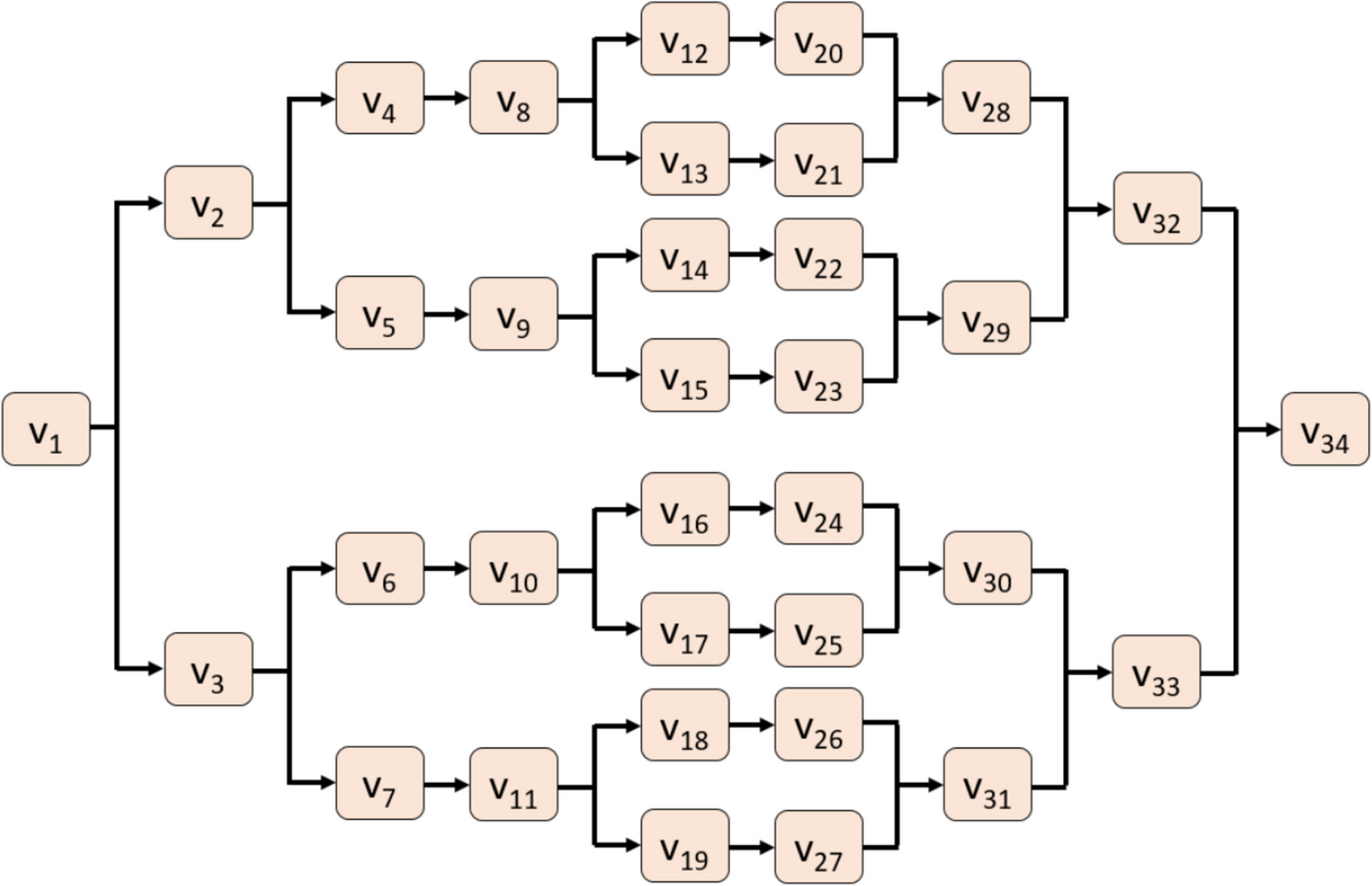
StrategiesThree possible strategies were developed, as depicted in Fig. 1. Strategy 1 is the current strategy with on-site decontamination and AMS in the CCP. Strategy 2 and 3 are novel strategies where contaminated victims receive their treatment and transport by PPE-donned healthcare workers, and decontamination is decentralized and organized by the hospitals themselves. Strategy 2 assumes 1 specific CBRNe MMT who performs on-site warm zone stabilization. Strategy 3 assumes no such MMT but assumes that every hospital has a specific team available at their decontamination unit to stabilize the patients before decontamination commences. In strategy 2 and 3, the treatment time is increased by 50% to account for the difficulties inherent in treating victims while wearing level B PPE [41, 42]. The AMS treatment time is based on real-life measurements from exercises and therefore already adjusted for PPE.
Fig. 1
Schematic overview of the victim path throughout simulated 3 strategies. Victims start at the incident site and end up either dead or in the emergency departments of the hospitals. There are three strategies simulated and both include the ‘Scoop and Run’ and ‘Stay and Play’ evacuation policies. The traffic lights represent a point of triage where the triage category of a victim might change. The smaller traffic light with only yellow and red lights represents the pretriage location
Evacuation PoliciesThere are two main policies implemented in the simulation model as described above: Scoop and Run and Stay and Play. These policies are simulated for every strategy.
Search and Rescue CapacityWe assume that all mobile victims left the station and either fled (wild evacuees) or are waiting to be examined at the top of the station at the CCP. Search and rescue at the subway station is performed by the HAZMAT teams of the Fire Service, who are the only personnel permitted to enter the contaminated station to evacuate incapacitated victims. Immobile victims arrive at the CCP based on a fixed inter-arrival rate of 5 min per S&R team consisting of 2 firefighters and a stretcher who perform the search and rescue procedure. There are 3 categories of S&R capacity: low (3 teams), medium (4 teams) and high (6 teams).
Patient Supervision during TransportDuring the transport phase, patients may be supervised in one of two ways: either by a pair of EMTs or by an MMT.
In the Belgian EMS system EMTs are limited to basic interventions such as oxygen administration, basic splinting and wound care. They are not allowed to administer IV fluids or drugs. Mobile Medical Teams are teams composed of an emergency physician and emergency nurse and can perform almost all advanced life support procedures on the scene. The Belgian EMS is designed to work in a tiered way, according to the needed level of care. A more detailed explanation of the Belgian EMS system can be found in appendix 2.
Two categories of transport supervision for T1/T2 patients have been implemented in the simulation:
EMT Supervision: Characterized by EMT-led supervision, this setting restricts the range of possible medical interventions during transport, thereby attenuating the overall treatment impact, as elaborated upon in the preceding treatment section.
MMT Supervision: Represents the normal HC112 operation standard where an MMT supervises the transport of seriously injured or ill patients.
Hospital AllocationThe simulation includes all hospitals located within a one-hour transport time radius. Each hospital’s capacity to receive T1 and T2 victims per hour—known as “surge capacity”—is self-reported and extracted from the hospital contingency plan. Furthermore, the specific medical capabilities of each hospital, such as neurosurgery, cardiothoracic surgery, and Level 1 trauma centers, are integrated into the hospital assignment algorithm. Some hospitals exclusively treat pediatric cases, while others possess distinct pediatric treatment capacities.
Prior to hospital transport, the Simedis score (SS) is evaluated to estimate each victim’s probability of surviving the transport. Victims with an SS less than 5 are presumed unlikely to survive transport. Two distinct hospital distribution policies have been implemented:
Closest First Policy: Prioritizes filling available hospital capacity based on their proximity to the incident site.
Spread Out Policy: Aims to distribute victims evenly across multiple hospitals in a round robin manner, thereby minimizing resource downtime at individual healthcare facilities.
Statistical AnalysisA sensitivity analysis determined that 10 simulator replications are adequate to get significant results. We created an ordinary least squares linear regression model to analyze the effect of every separate parameter on the prehospital mortality which is our primary outcome variable. The analysis was performed with the python package statsmodels [43].
Comments (0)