
Remember me








The clinical characteristics of all patients are shown in Table 1. The median age at treatment was 64 years (range, 29–86). The most predominant histological type was papillary RCC (43.2%), followed by translocation RCC (13.6%), and then mucinous tubular and spindle RCC (9.1%). With respect to the IMDC risk classification, 9%, 57%, and 34% were classified as favorable-, intermediate-, and poor-risk, respectively. Nephrectomy had been performed in 24 patients (54.5%). The most common sites of metastasis were lymph nodes in 25 cases (56.8%), followed by lung in 20 cases (45.5%), bone in 12 cases (27.3%), and liver in 11 cases (25.0%) (Supplementary Table 1).
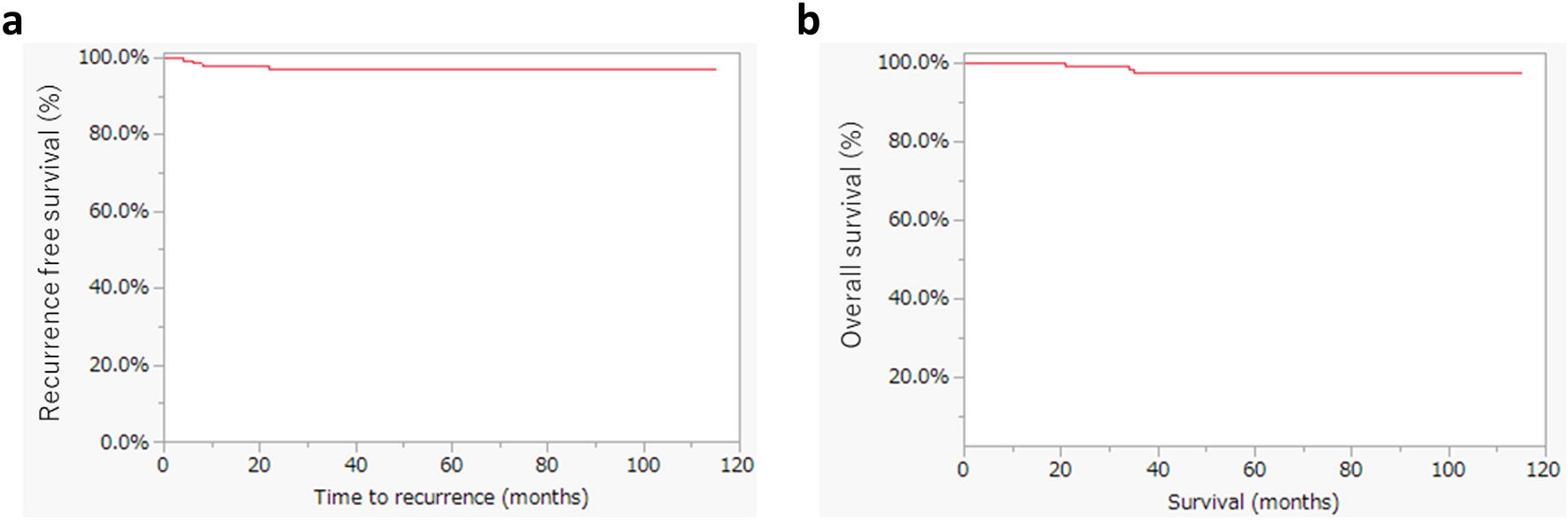
Table 1 Baseline characteristics of nccRCC patientsClinical outcomes of metastatic nccRCC patients with combination therapyThe median duration of first-line ICI combination treatments was 5.8 month (range, 0.2–54.9), and the median follow-up period was 15.2 month (range, 0.2–54.9). During the observational period, 27 patients (61.4%) died from cancer. Overall, the median OS was 23.9 months, and the median PFS was 8.8 months (Fig. 1). Among 44 patients, CR and PR were achieved in 0 and 16 patients (36.3%) and SD was observed in 17 patients (38.6%), resulting in objective response rate (ORR) of 36.3% and disease control rate (DCR) of 75.0% (Fig. 2).
Fig. 1
Kaplan–Meier survival curves for all metastatic nccRCC patients treated with ICI combination therapy. A Progression-free survival (PFS). B Overall survival (OS)
Fig. 2
Response rates in nccRCC patients with ICI combination therapy. There were no patients with CR in this study. The ORR of ICI + TKI group, ICI + ICI group and all cases was 41.6%, 30.0% and 36.3%, respectively. The DCR was 79.2%, 70.0% and 75.0%, respectively
Next, we investigated the regimen of ICIs combination therapies affected clinical outcomes in our cohort. Importantly, there was no significant difference in PFS and OS between ICI + TKI and ICI + ICI groups (p = 0.778 and p = 0.559, respectively) (Fig. 3). Even when limited to the patients with papillary RCC, there was no statistically significant difference between two groups in terms of PFS and OS (p = 0.556 and p = 0.676, respectively) (Supplementary Fig. 1).
Fig. 3
Survival analysis for patients nivolumab plus ipilimumab and anti-PD-1/PD-L1 inhibitor plus tyrosine kinase inhibitors. Kaplan–Meier survival curves showing A progression-free survival (PFS) and B overall survival (OS) between nivolumab plus ipilimumab (ICI + ICI group) and anti-PD-1/PD-L1 inhibitor plus TKI (ICI + TKI group). PFS and OS were similar in both groups (8.8 months versus 6.4 months, p = 0.778 and 26.8 months versus 23.9 months, p = 0.559, respectively)
Since there were no patients with favorable risk in the ICI + ICI group, we performed the additional analysis after excluding patients with favorable risk in the ICI + TKI group. As a result, there was no significant difference in PFS and OS between two groups (p = 0.776 and p = 0.433, respectively) (Supplementary Fig. 2).
Clinical outcomes of patients with cabozantinib immediately after combination therapy as the second-line therapyWe further aimed to evaluate the efficacy of TKIs immediately after discontinuation of ICIs combination therapies. As shown in Table 1, the most common treatment after the combination therapies was cabozantinib (36.3%). The median PFS was 6.8 months in these patients (Supplementary Fig. 3). Among them, CR and PR were achieved in 1 (6.3%) and 2 patients (12.5%), and SD was observed in 6 patients (37.5%), resulting in the ORR of 18.8% and the DCR of 56.3% (Supplementary Table 2). In contrast, in patients with other types of TKIs, the ORR and DCR were 14.3% and 28.5%, respectively.
Safety analysisSpecific details regarding the AEs reported in our study are shown in Table 2. In the present study, any grade and grade 3–5 immune-related AEs (irAEs) occurred in 16 (36.3%) and 9 (20.5%) patients. Two patients with pneumonitis experienced grade 5 irAE. They were treated with nivolumab plus cabozantinib. The most frequent irAEs were related to hepatitis (13.6%) followed by adrenal insufficiency (9.0%) and pneumonitis (9.0%). All irAEs except grade 5 were recovered, although 4 patients with adrenal insufficiency required continuous corticosteroid therapy. The most common AE caused by TKI was fatigue (20.8%), followed by hand-foot syndrome (12.5%) and hepatitis (12.5%). All patients with AEs induced by TKIs showed improvement upon discontinuation of the medication. During the observational period, 9 patients discontinued the combination therapy due to the occurrence of AEs. Importantly, there was no significant difference in the percentage of discontinuations due to AEs between the ICI + ICI group and the ICI + TKI groups (15.0% versus 25.0%, p = 0.413, Fig. 4A).
Table 2 Summary of AEs in nccRCC patients with ICI combination therapyFig. 4
Percentage of patients who discontinued treatment because of adverse events. A There was no significant difference in the percentage of discontinuations due to adverse events (AEs) between the ICI + ICI group and the ICI + TKI groups (15.0% versus 25.0%, p = 0.413). B The discontinuation rate of treatment due to AEs in patients aged ≥ 75 years was significantly higher compared to that in patients aged < 75 years (45.5% versus 12.2%, p = 0.017). irAE; immune-related adverse event
Recently, the efficacy and safety of ICI combinations therapy in elderly patients with ccRCC have been reported [18, 19]. In our cohort, 25.0% of patients were aged ≥ 75 years. When patients were stratified into two groups according to their age (≥75 years or <75 years, n = 11 and n = 33), the incidence of AEs did not differ between the two groups (63.6% versus 48.5%, p = 0.384). Although the discontinuation rate of the combination therapy due to AEs in patients aged ≥ 75 years was significantly higher compared to that in patients aged < 75 years (45.5% versus 12.2%, p = 0.017) (Fig. 4B), there were no significant differences in PFS and OS between two groups (p = 0.290 and p = 0.257, respectively) (Supplementary Fig. 4).
Correlation between the clinicopathologic factors and clinical efficacyWe further investigated the impacts of several clinicopathologic factors on PFS and OS in metastatic nccRCC patients with ICIs combination therapy (Table 3 and Table 4). Univariate analysis revealed that female gender and liver metastasis were significantly associated with the decrease of PFS. Interestingly, multivariate analysis also demonstrated that female and the presence of liver metastasis were both significantly associated with worse PFS. With respect to OS, univariate and multivariate analysis also revealed that the presence of liver metastasis had significant association with worse OS.
Table 3 Univariate and multivariate Cox proportional hazards regression analysis for the prognostic factors of PFS (n = 44)Table 4 Univariate and multivariate Cox proportional hazards regression analysis for the prognostic factors of OS (n = 44)
Comments (0)