Study design and participants
This is a multicenter prospective randomized controlled 2-arm parallel trial. Between September 2020 and January 2022, patients were recruited from four academic tertiary care centers: Beijing Tiantan Hospital, Capital Medical University (Beijing City, China); Renji Hospital, Shanghai Jiaotong University School of Medicine (Shanghai City, China); Suzhou Municipal Hospital (Suzhou City, Jiangsu Province, China); and Sir Run Run Shaw Hospital (SRRSH), Zhejiang University School of Medicine (Hangzhou City, Zhejiang Province, China). The study was conducted according to the principles of the Declaration of Helsinki and approved by the ethics committees of all participating centers.
Women were eligible if they were aged 18–40 years, diagnosed with moderate-to-severe IUA (American Fertility Society (AFS) score greater than or equal to 5 points) under hysteroscopy, and volunteered to receive the intrauterine estrogen-releasing system (experiment arm) or a Foley catheter balloon combined with oral estrogen therapy (control arm) after TCRA. Women were excluded if they were contraindicated for TCRA, used high-dose estrogen drugs within 1 month before surgery, or simultaneously suffered from genital tuberculosis, acute genital inflammatory disease, abnormal uterine bleeding, malignant tumors, or other systemic disease, such as chronic cardiocerebrovascular, liver, kidney, hematopoietic system, or psychiatric disorders. All enrolled participants provided written informed consent and agreed to the study protocol before the intervention.
Randomization and blinding
Eligible women were identified by the principal investigators in the participating centers and consented women were allocated in a 1:1 ratio to one of the two treatment arms. Enrollment at each center was performed with the use of blocks, and the participants were randomized for sample balance. SAS 9.4 software was used to generate a random assignment table. Because of the nature of the intervention, it was not possible to blind the participants or their treating doctors to the allocated treatment.
Interventions
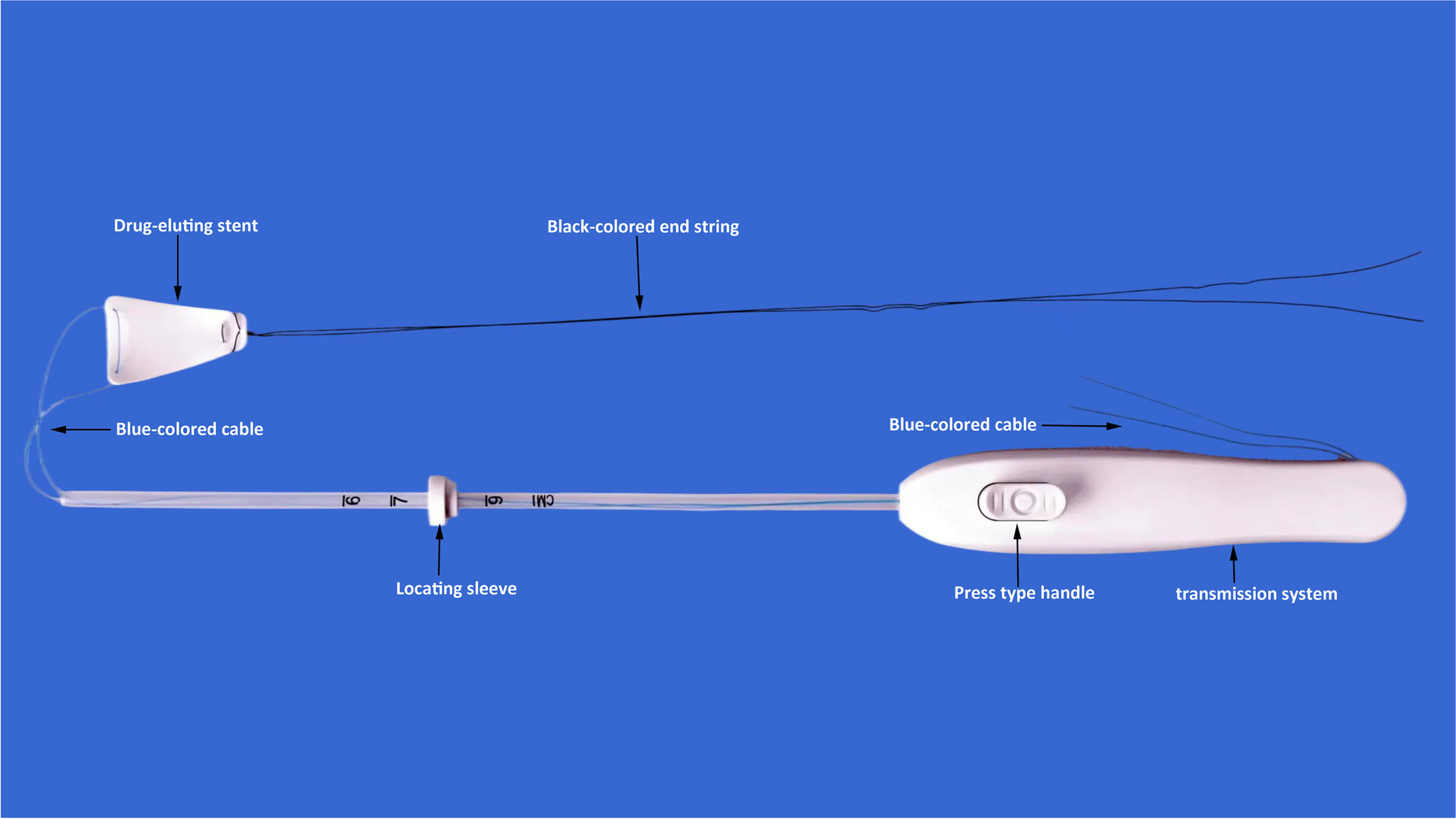
TCRA was performed by the same surgical team at each independent center (n = 4 teams total). After TCRA, patients in the experimental group received a silicone rubber intrauterine stent system to prevent adhesion reformation, while the control group received a Foley catheter balloon combined with self-crosslinked sodium hyaluronate gel and cyclic estrogen-progestin therapy. In the experimental group, the silicone rubber intrauterine stent system was removed 60 days after TCRA, followed by a consecutive 5-day course of dydrogesterone at 20 mg/day. Sequential estrogen-progestin therapy was administered to the control group for two cycles following the TCRA, which consisted of continuous use of estradiol valerate tablets (6 mg/day) for the first cycle, followed by the addition of dydrogesterone tablets (20 mg/day) for the second half, or continuous use of estradiol valerate tablets for 60 days (6 mg/day), followed by dydrogesterone tablets (10 mg/day) for the last 10 days (as dictated by surgical team preference).
Outcome variables
The primary outcome of this study was the rate of adhesion reduction at 60 days postoperatively. Adhesion reduction was defined as a decrease of ≥ 4 points based on AFS under hysteroscopy [8]. The severity of IUA is also evaluated by the criteria of the European Society of Gynecological Endoscopy (ESGE) classifications under hysteroscopy.
The secondary outcomes were other efficacy and safety indicators, which included endometrial thickness at the period of ovulation, menstrual improvement rates, serum estradiol levels, daily estradiol release, pregnancy rates, and other reported adverse events during follow-up.
Endometrial thickness (during the ovulation period) was evaluated through three-dimensional transvaginal ultrasound before and 60 days after surgery. Postoperative improvements in menstruation were assessed using the Pictorial Bleeding Assessment Chart (PBAC) score.
Serum estradiol levels were evaluated at 24 h, 72 h, 14 days, 30 days, and 60 days postoperatively. The remaining drug content in the intrauterine stent was evaluated 60 days after surgery. The daily release amount was calculated as the total release amount divided by the number of days of implantation.
Pregnancy rates were assessed 1-year post-surgery. Other adverse events including uterine perforation, postoperative bleeding, pain, genital tract infection, liver or kidney injuries, and coagulation abnormalities were evaluated with CACTE 5.0 until 60 days postoperatively.
Statistical analysis
Statistical analysis was performed using SAS 9.4 statistical analysis software. All the statistical tests were two-tailed (unless otherwise specified), and a p value less than 0.05 was considered to indicate statistical significance. Mean differences were compared using paired t-test (when tests of normality and homogeneity of variance were satisfied), and categorical data were analyzed using chi-squared or Fisher’s exact probability tests (when a chi-squared test was inappropriate). Ranked data were analyzed using the Cochran-Mantel–Haenszel (CMH) test.






Comments (0)