
Remember me
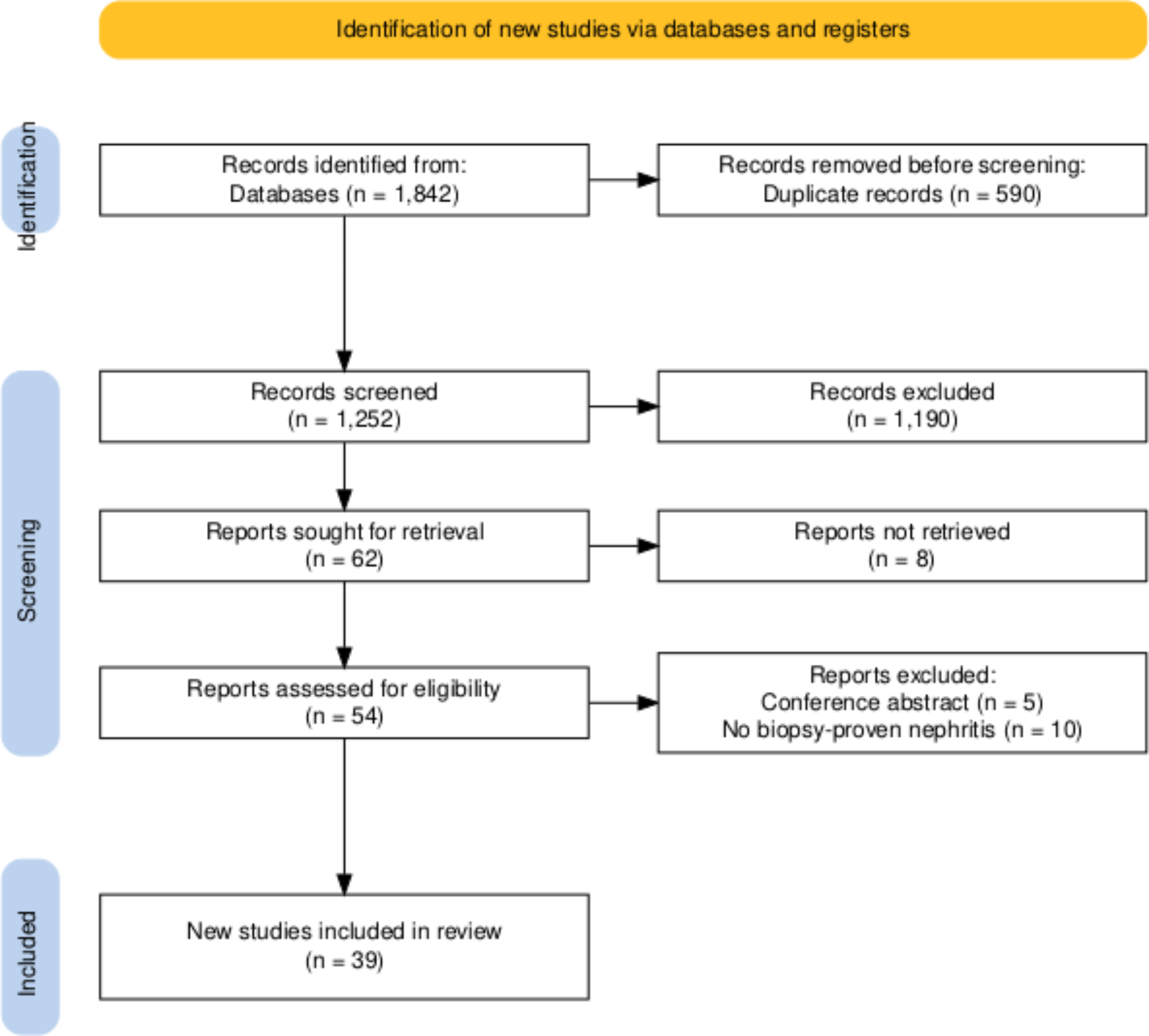
In total, 97 patients were included in the study, and 31 patients were excluded (Fig. 1); forty-two (43.3%) were female and 55 (56.7%) were male. The median age was 66 years (interquartile range [IQR], 56–79 years), and 17 patients (17.5%) were admitted to the intensive care unit. Examining the comorbidities of participating patients, 58 (59.8%) had two or more comorbidities. Online Resources 1 and 2 present the underlying comorbidities for the viral and BSI groups. Eleven patients died during their inpatient stay.
Baseline characteristics of patients with BSIBSI was diagnosed in 56 patients (57.7%) (Fig. 1). In total, 19 different bacterial species and two Candida species were identified. The most common bacterial pathogens were Escherichia coli (E. coli) (18 patients, 32.1%) and Klebsiella pneumoniae (8 patients, 14.3%). Blood cultures were simultaneously positive for two bacterial species in seven patients. In three patients, blood cultures were simultaneously positive for three different bacterial species. Online Resource 3 presents the bacterial species detected.
The most common sources of BSI were urogenital and urinary (18 patients, 32.1%), abdominal (7 patients, 12.5%), and soft tissue (7 patients, 12.5%) infections. Ten patients (17.9%) developed neutropenic fever because of chemotherapeutic treatment for underlying haemato-oncological malignancies (Table 1). The median CRP level was 11.9 (interquartile range [IQR], 7.5–21.7) mg/dL; PCT, 2.4 (IQR, 0.6–13.3) ng/mL; and white blood cell count (WBC), 7.0 (IQR, 2.8–12.6) G/l. PCT values were collected at an interval of zero (IQR 0–1) days from the values of the host-protein signature score.
Table 1 Sources of bacterial infection in patients with blood stream infectionAll 56 patients with BSI received antibiotic treatment. Following our SOC, antibiotic therapy was initiated at a median of 1 day (IQR, 1–2 days) ahead of positive blood culture results because of suspected bacterial infection. Among the 56 patients with BSI, one did not receive antibiotic treatment before the blood culture became positive, as per SOC. This patient had a score of > 65 and would, therefore, have received antibiotic treatment earlier compared to the SOC.
The most common comorbidities were arterial hypertension (31 patients, 55.4%), diabetes mellitus (12 patients, 21.4%), atrial fibrillation (10 patients, 17.9%), and coronary artery disease (10 patients, 17.9%). Six patients (10.7%) received immunosuppressive therapy at the time of BSI. Two patients (3.6%) previously received an organ or stem cell transplantation, respectively (Online Resource 1).
Results of the host-protein signature score and PCT in patients with BSIIn patients with BSI (56 patients), the median host-protein score was 99 (IQR, 89.8–100). In total, 49 patients (87.5%) had a score > 65. In four patients (7.1%), the probability of a viral or bacterial infection was considered equivocal, with a score ranging from 36 to 65. Three patients (5.4%) with BSI had a score < 35, indicating the absence of a bacterial infection. (Fig. 2) The overall sensitivity for the score for identifying BSI was 87.5%. (Table 2) After excluding immunocompromised patients, sensitivity for the score for identifying BSI was 91.9%. (Table 3) PCT data were available for 47 patients (83.9%). The median PCT in patients with BSI was 2.4 ng/mL (IQR, 0.6–13.3 ng/mL). Using a cut-off of > 0.5 ng/mL, PCT demonstrated a sensitivity of 76.6% in detecting BSI. (Table 2). After excluding immunocompromised patients, sensitivity for PCT was 93.3%. (Table 3)
Fig. 2
Graphical overview of the total cohort with host-protein signature score results
Table 2 Quality criteria of the host-protein signature score and PCTTable 3 Quality criteria of the host-protein signature score and PCT in immunocompetent patientsAmong patients with a score > 65, 17 (34.7%) were tested positive for E. coli, 8 (16.3%) for Klebsiella pneumoniae, and six (12.2%) for Staphylococcus aureus (Online Resource 3). Immunosuppressive therapy was received by four patients (8.2%) (Online Resource 1). The median duration between initiation of antibiotic therapy and the score was 2 days (IQR, 1.0–3.0 days).
In the four patients with a score ranging from 35 to 65, the pathogens isolated from blood cultures were Staphylococcus epidermidis, Enterococcus faecium, Streptococcus anginosus, and Proteus mirabilis (Online Resource 3). One patient (25.0%) was receiving immunosuppressive therapy (Online Resource 1). The median duration between initiation of antibiotic therapy and the CLIA was 3.5 (IQR, 0.75–4) days. PCT data were available for two patients, with a median of 11.2 ng/mL.
In the three patients with a score < 35, the detected bacterial species were Staphylococcus epidermidis, Staphylococcus hominis, and E. coli (Online Resource 3). These were diagnosed in two cases of central catheter infections and urosepsis. One patient was receiving immunosuppressive therapy (Online Resource 1). All patients were treated with antibiotics, with a median time of 2 days before the CLIA. Data on PCT levels were available for two patients, with a median of 0.3 ng/mL.
Baseline characteristics of patients with viral infectionsA viral infection with negative blood culture results was diagnosed in 41 patients (Fig. 1). Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was the most commonly detected virus (24 patients, 58.5%). Influenza A/B was detected in 11 patients (26.8%) and respiratory syncytial virus (RSV) in seven patients (17.1%). One patient (2.4%) was diagnosed with human metapneumovirus, and one with dengue virus. Three patients (7.3%) were diagnosed with two viruses (Influenza A/RSV and Influenza A/SARS-CoV-2) simultaneously (Table 4). The median CRP was 8.6 (IQR, 6.1–14.5) mg/dL; PCT, 0.2 (0.1–1.2) ng/mL; and WBC 6.0 (IQR, 4.0–9.0) G/l. PCT values were collected at an interval of zero (IQR 0–1) days from the values of the host-protein signature score.
Table 4 Viral pathogens detected in patients with viral infectionsFollowing our SOC, 31 (75.6%) patients without BSI but with viral infections received antibiotic treatment, with a median of 1.5 days (1–2 days) before the CLIA. One patient (2.4%) received routinely administered antibiotic treatment after peroral endoscopic myotomy; there was no evidence of a bacterial infection. Table 5 illustrates the rationale for the antibiotic treatment. In 17 patients (53.1%), a pulmonary bacterial superinfection was suspected on diagnostic imaging, three patients had an additional bacterial urogenital focus (9.4%), three patients (9.4%) received antibiotic treatment due to neutropenic fever, two (6.3%) had a bacterial soft tissue infection, and one (3.1%) had a suspected cholangitis. In five patients with cancer (15.6%), calculated antibiotic therapy was administered owing to immunosuppression with distinctly increased infection markers and/or severe course of disease (low oxygen saturation/intubation) (Table 5).
Table 5 Reasoning behind antibiotic treatment in patients with primarily viral infections and without blood stream infection in relation to the host-protein signature scoreThe most common comorbidities were arterial hypertension in 13 patients (31.7%) and atrial fibrillation in nine patients (22.0%). In total, 12 patients (29.3%) were receiving immunosuppressive therapy, and two patients (4.9%) were receiving B-cell depletion. Six patients (14.6%) underwent stem cell or organ transplantation (Online Resource 2).
Host-protein signature score results in patients with viral infectionsIn total, 41 patients without BSI but with viral infections were included, and the median score was 90 (IQR, 13.5–98). Twenty-nine patients (70.7%) exhibited a score of > 65, while one patient (2.4%) had a score ranging from 35 to 65, and eleven patients (26.8%) had a score of < 35. (Fig. 2) Twenty-nine patients had a score > 65 and should have received antibiotic therapy according to the manufacturer’s recommendation. Of these 29 patients, 25 (86.2%) received antibiotic treatment following our SOC. Thus, four out of 29 patients with a score > 65 (13.8%) did not receive antimicrobial treatment, as no bacterial super/coinfection was suspected based on clinical assessment. These four patients, who were not treated with antibiotics following SOC, had respiratory infections: three cases of SARS-COV-2 and one of RSV. These patients’ mean PCT and CRP values were 0.87 ng/mL and 8.83 mg/dL, respectively. None of these patients died or required intensive care.
The patient with a score between 35 and 65 got antibiotic treatment due to an underlying oncological disease with immunosuppressive medication. In patients with a viral infection and a score < 35, SOC resulted in antibiotic treatment for suspected bacterial infection in six of eleven patients. In three of these six patients, a respiratory bacterial superinfection was suspected on diagnostic imaging; two patients were additionally diagnosed with a urogenital infection, and one had neutropenic fever. (Table 5) No patient died or required intensive care. PCT data were available for eight of eleven patients (72.7%), with a median of 0.1 (IQR, 0.1–0.4) ng/mL.
Comments (0)