
Remember me
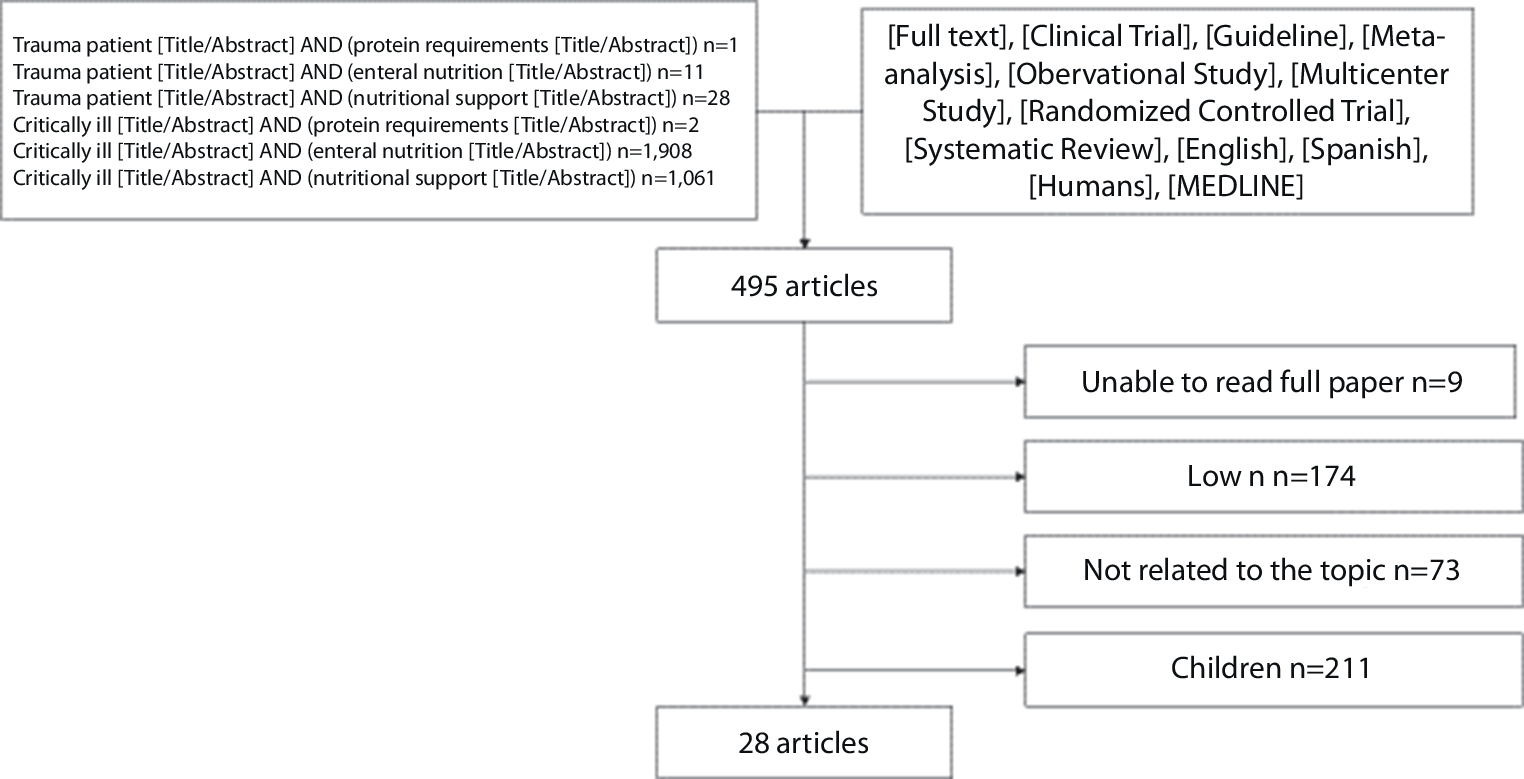



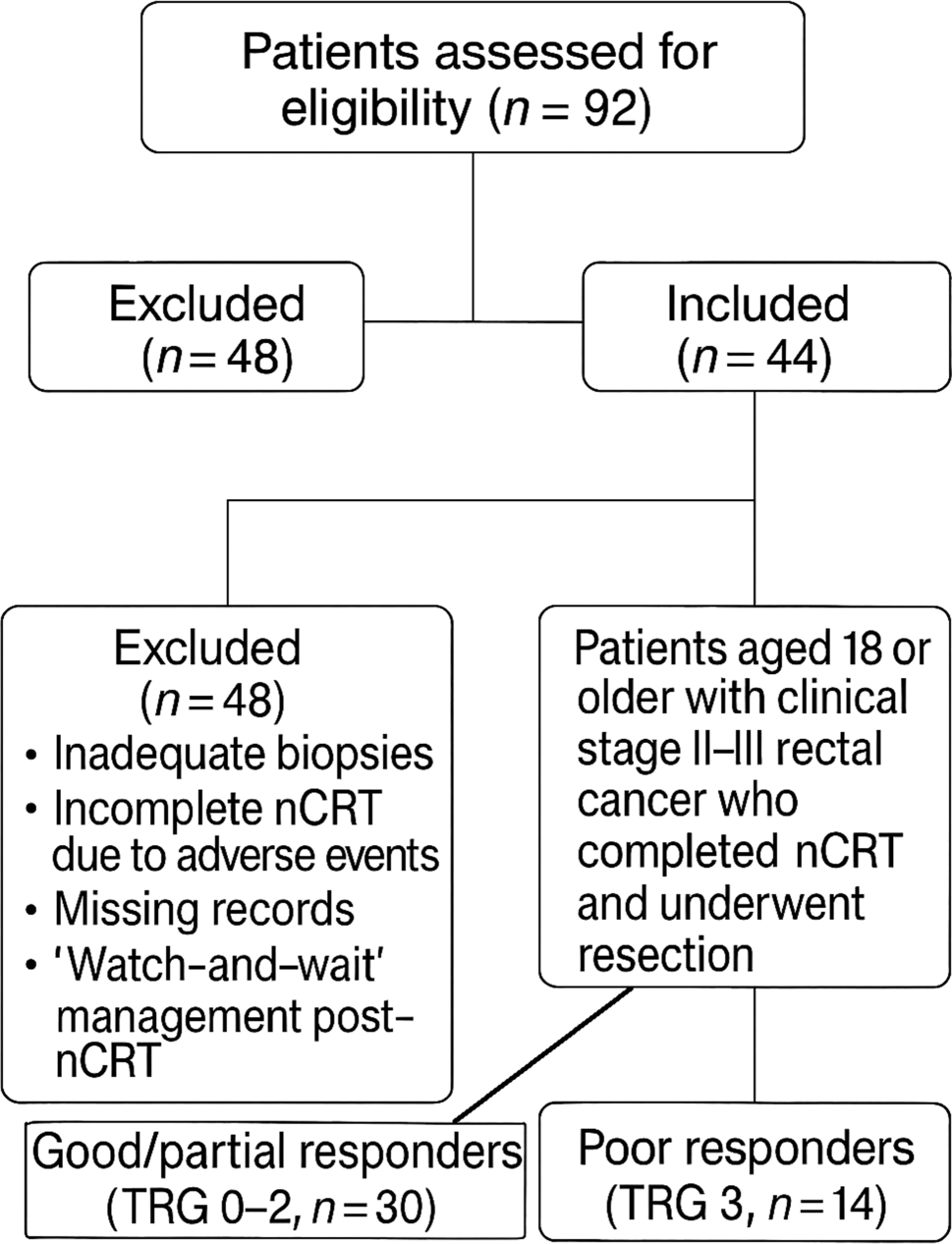

A total of 2524 records were identified through searching databases, of which 1675 were screened after removal of duplicates. During screening, 1572 records were excluded, and 103 full-text articles were assessed for eligibility. Eight additional records were identified through citation searching, of which seven were assessed for eligibility. In total, 63 articles (with data from 40 RCTs) met the inclusion criteria and were included [14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76]. The flow diagram (Fig. 1) shows the work process for study selection and reasons for exclusion of full-text articles.
Fig. 1
Search results and workflow of study selection
Included studiesCharacteristics of included studies are summarized in Table 1. This systematic literature review included a total of 2619 participants treated with LNF. When presented, the study population was comprised of between 37% and 75% men, with a mean age of 42.9 to 59.1 years (median 42.5 to 52.0 years). The studies were conducted on five continents, mostly in Europe, and published between 1997 and 2022. Without further description, the comparator was one of the following: open Nissen fundoplication [14, 27, 29, 33, 36, 42, 74], laparoscopic Hill repair [19], laparoscopic anterior 90° fundoplication [57, 72], laparoscopic 120° anterior fundoplication [28], laparoscopic 180° anterior fundoplication [20, 25, 56, 65], laparoscopic 200 to 270° (Toupet) fundoplication [24, 35, 37, 40, 41, 44, 46, 55, 59, 60], robot-assisted LNF [32, 48, 49, 52], laparoscopic Lind fundoplication [39], a variation of LNF [22, 26, 34, 53, 54, 61, 69], or PPI therapy [15, 16, 45]. For the included studies with a variation of LNF, only one was considered as the intervention group and included in this review. The variations considered to be the comparator group and not presented in this review included LNF without division of short gastric vessels [22, 26, 61], LNF with crural closure using simple sutures and mesh hiatoplasty [34], additional prosthetic hiatal closure with a bougie [54], additional anterior hiatal closure [69], and LNF with suturing of the wrap to both diaphragmatic crura or to the body of the stomach [53]. In one study, the intervention group was divided into LNF with a 1.5- or 3‑cm wrap, but only data for participants receiving a 3-cm wrap were included [46, 47].
Table 1 Characteristics of included studiesIntraoperative outcomesAll included studies presented results for at least one intraoperative outcome (Table 2). In total, 78 injuries and other complications occurred. Most were respiration-related complications (4.5%), followed by bleeding (2.9%). Furthermore, 39 cases (1.6%) required conversion to open surgery, reported by 37 articles. Gastroesophageal injury or perforation occurred in 0.9% of the subjects, reported by 17 articles. However, no deaths occurred during LNF surgery. As shown in Table 2, several outcomes were sporadically reported by the included studies, except for conversion to open surgery.
Table 2 Number of intraoperative eventsPostoperative outcomesHeartburn and epigastric/sternal pain were combined into one outcome measure for the purposes of this review, which is referred to as “heartburn or epigastric/sternal pain” from this point on. Appendix B presents some results in more detail.
Results from the two earliest postoperative timepoints were collated into one period, i.e., 4 to 6 weeks after surgery. A summary of postoperative results is shown in Table 3 and presented more elaborately in Supplementary Table B.2. In total, 15 studies reported some result among 656 participants [14, 28, 34, 39, 48, 49, 52,53,54, 57, 60, 61, 69, 72, 75]. Postoperative events were common, particularly dysphagia (46.1%), gas bloating (32.5%), and heartburn or epigastric/sternal pain (31.9%).
Table 3 Summary of clinical postoperative events at 4 to 6 weeks, 6 months, 1 year, 5 years, and 10 years follow-upaAt 6 months, some postoperative events decreased in frequency while others increased among the 584 available participants from 13 of the included studies [14, 22, 24,
Comments (0)