
Remember me









This was a randomized, double-blind, placebo and reference controlled, double-dummy, dose-finding, parallel-group, multicenter, international, prospective study that was performed in 30 investigational sites in four countries (Czech Republic, France, Poland, and the United Kingdom). The EudraCT trial number was 2018-000133-12, while the Clinical Trial registration is NCT03749642. The study was approved by the Competent Authorities and applicable Ethic Committees of Czech Republic (State Institute for Drug Control, Thomayerova nemocnice a IKEM, Ethics Committee Nemocnice Pardubického kraje a.s., Axon Clinical, Etická komise CLINTRIAL s.r.o.), France (ANSM Agence Nationale de Sécurité du Médicament et des produits de santé and Comité de Protection des Personnes (CPP) désigné par le système CNRIPH), Poland (Departament Badań Klinicznych Produktów Leczniczych Urząd Rejestracji Produktów Leczniczych, Wyrobów Medycznych i Produktów Biobójczych and Komisja Bioetyczna przy Śląskiej Izbie Lekarskiej w Katowicach), and United Kingdom (Medicines and Healthcare products Regulatory Agency and East of England—Cambridgeshire and Hertfordshire Research Ethics Committee) and was conducted in accordance with Good Clinical Practice guideline and ethical standards as laid down in the 1964 Declaration of Helsinki. Written informed consent (including personal data processing) was obtained from all individual participants included in the study prior starting any study-related procedure. The study consisted of three main study periods: the screening and wash-out, the 8-week double-blind investigational treatment period, and the 8-day tapering period, for a maximum of ten visits (Fig. 1).
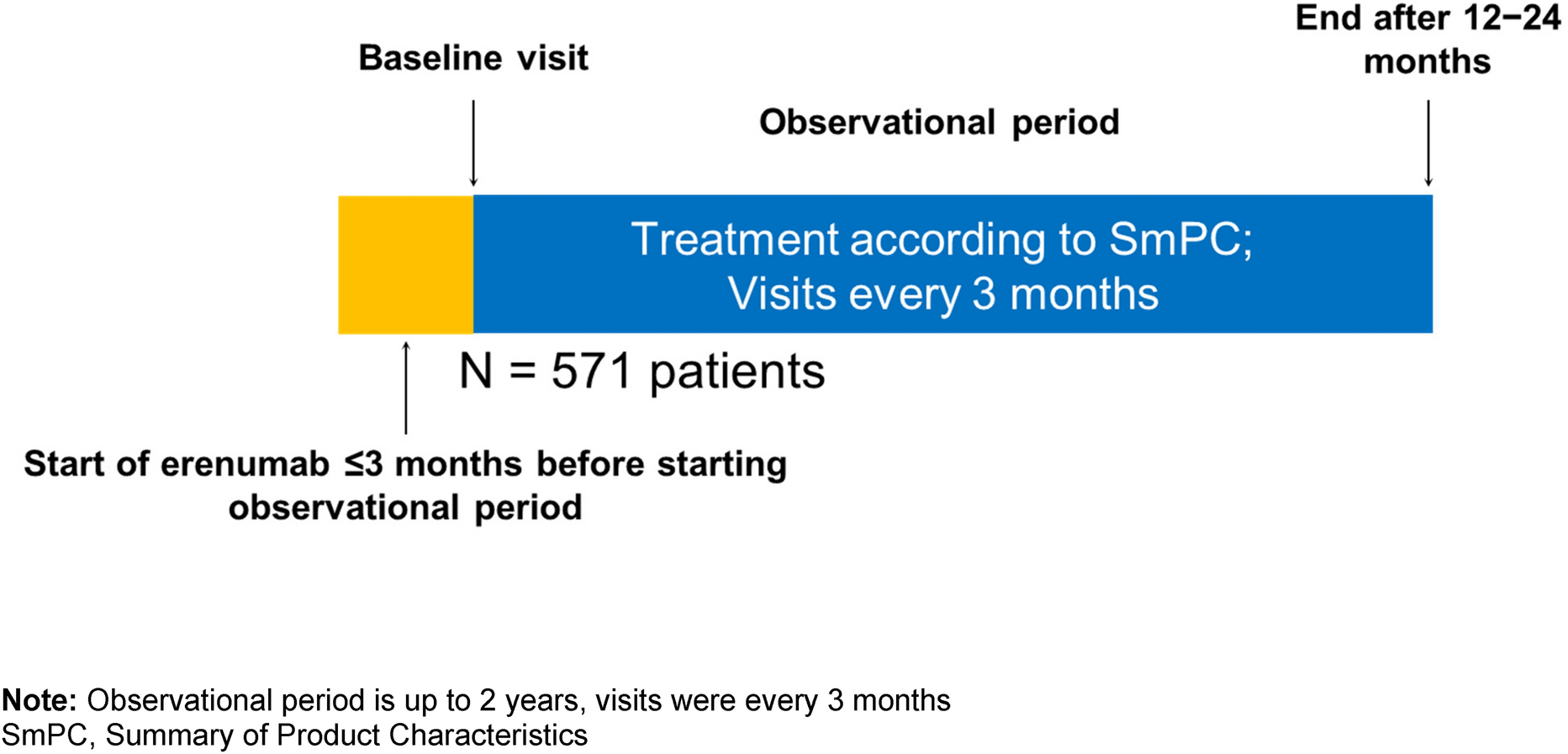
Fig. 1 Participants
ParticipantsThe patients were eligible to enter the study if the following main inclusion criteria were met: male or female patient between 18 and 75 years of age (limits included); neuropathic pain at feet/legs confirmed by DN4 score ≥ 4 at screening visit; bilateral distal symmetrical polyneuropathy confirmed by Toronto Clinical Neuropathy Scoring System (TCNSS) score > 5 at screening visit; pain persisting or taking pain medication for neuropathic pain for at least 3 months; diabetic patient (type 1 or 2 diabetes mellitus) with value of HbA1c ≤ 11% at screening visit and stable antidiabetic medication regimen for ≥ 30 days; patient who was currently not receiving treatment for diabetic neuropathic pain or patient who was receiving treatment, with drug/s other than gabapentin, and had completed the required washout; average daily pain score ≥ 4 based on the 11-point NRS at visit 0, calculated from a minimum of four pain ratings in daily electronic device entries during the baseline period; women of childbearing potential with a negative pregnancy test at screening visit; patients legally capable to give their consent to participate in the study and available to sign and date the written informed consent (including personal data processing). Main exclusion criteria included: known hypersensitivity to trazodone or gabapentin or any excipients of the test drugs, other form of non-diabetic distal symmetric polyneuropathy or any other pain condition that could impair the study endpoints; concomitant treatment with other medications for pain management; use of trazodone or gabapentin in the previous 3 months; active foot ulcer or previous major limb amputation; glomerular filtration rate (GFR) value < 50 ml/min calculated with Modification of Diet in Renal Disease (MDRD) formula; significant mental disorders.
At each clinical site, investigators, who were mainly neurologists with experience in managing patients suffering from PDN, were responsible for assessing the eligibility of the patients including diagnosis and all related criteria.
A total of 240 evaluable patients were planned to be enrolled in the study and randomized to one of the following treatment groups in double-blind condition:
Group 1: Trazo/Gaba 2.5/25 mg, capsules, t.i.d. for 8 weeks.
Group 2: Trazo/Gaba 5/50 mg, capsules, t.i.d. for 8 weeks.
Group 3: Trazo/Gaba 10/100 mg, capsules, t.i.d. for 8 weeks.
Group 4: Gaba, capsules, administered as per Summary Product Characteristics (SPC) up to the maximum dosage of 1800 mg daily.
Group 5: PLB, capsules, t.i.d. for 8 weeks.
After the 8-week treatment period, patients allocated into the Gaba group started 8 days of tapering off in double-blind conditions. Thus, patients allocated in the other groups received an 8-day tapering period with PLB in order to maintain the double-blind conditions.
During the study, medications for pain management, including but not limited to tricyclic antidepressants, serotonin, and norepinephrine reuptake inhibitors, other GABA analogue different from gabapentin, opioids, mexiletine hydrochloride, carbamazepine, phenytoin, valproate sodium, dextromethorphan, capsaicin, corticosteroids, nonsteroidal anti-inflammatory drugs, skeletal muscle relaxants, benzodiazepines, and over-the-counter medications with centrally acting properties were prohibited and had to be discontinued for a period specific to the taper schedule (based on five elimination half-lives of the used medication) before randomization. In case of need, only paracetamol as analgesic and aspirin for prophylaxis of myocardial infarction or transient ischemic attack were allowed.
Randomization and blindingAt visit 0 (baseline, day 0) patients fulfilling eligibility criteria were randomly assigned to receive Trazo/Gaba 2.5/25 mg, or Trazo/Gaba 5/50 mg, or Trazo/Gaba 10/100 mg, or Gaba, or PLB, in a 1:1:1:1:2 ratio. To randomize patients, investigators were properly directed to assign the product following the sequential order of the randomization number reported on the label of each patient’s drug package. The randomization scheme was a computer-generated sequence. Before supplying the investigational drug to clinical sites, all the test drugs were covered in anonymous DB AA-EL capsules in order to maintain the double-blind condition of the study. In case of a medical emergency, the investigator was able to unblind the treatment code through the blinded labels provided by the sponsor.
Study Outcome MeasuresThe primary end point of the study was the change from baseline of the average daily pain score based on the 11-point NRS (“from 0 = no pain to 10 = worst possible pain”) after 8 weeks of treatment (visit 6, day 56 ± 2). At baseline and each subsequent time point, the scores were averaged from the last seven entries done by patients in the electronic device, calculated from a minimum of four pain ratings.
As secondary endpoints, this study assessed the following parameters: change from baseline of 11-point NRS at each other visits; % of responders (defined as ≥ 30% and ≥ 50% reduction from baseline of the average daily 11-point NRS; the neuropathic pain symptoms using the Neuropathic Pain Symptom Inventory (NPSI) and BPI-SF; anxiety and depression using the Hospital Anxiety and Depression Scale (HADS) and Beck Depression Inventory—Second Edition (BDI-II); sleep using the Insomnia Severity Index (ISI); quality of life using the Euroqol-5D-5L (EQ-5D-5L); safety and tolerability.
Among the pain rating scales, the 11-point NRS has been extensively used and validated as pain is always subjective and self-assessment scale provides the most valid measure of the experience [18]. BPI-SF has been specifically validated for PDN [19], while NPSI is a validated self-questionnaire designed to evaluate the different symptoms of neuropathic pain [20]. BDI-II consists of 21 items to assess the intensity of depression in clinical and normal patients [21], while HADS is commonly used to assess the level of anxiety and depression that a patient is experiencing [22]. ISI is a seven-item self-reported instrument measuring the patient's perception of his/her insomnia targeting the severity of symptoms, the consequences of insomnia, as well as the degree of distress caused by those difficulties [23, 24]. EQ-5D-5L is based on self-report of five domains: mobility, self-care, usual activities, pain and discomfort, anxiety and depression, plus a visual analogue scale (VAS) that records the patient’s self-rated health on a vertical scale [25]. CGI-C provides a global rating of patient’s improvement [26].
As safety variables, adverse events were monitored throughout the whole study from the signature of the informed consent up to the last study visit. A complete physical examination (including the measurement of vital signs) was performed at all visits, while laboratory analysis (hematology, serum chemistry, and urinalysis) were done at the screening visit, visit 4, and visit 6. Blood and urine samples were analyzed by the Central Laboratory ACM located in UK and lab reports were assessed by the investigator. The patients were also monitored for the cardiac safety at the screening visit, visit 1, visit 4, visit 5, and visit 6: 12-Lead ECGs were evaluated by the Central Cardiac Laboratory Bioclinica located in US.
Statistical AnalysisThe sample size of this study was calculated supposing a linear relationship between dose and response, using the linear contrast method, with an unequal allocation, duplicating the PLB arm to increase the power of the study [27]. A total of 200 patients with a ratio 2:1:1:1 (80 patients for the PLB group and 40 for the other Trazo/Gaba groups) was required to detect a difference in the primary endpoint, supposing an effect of − 2 for PLB, − 2.25 for Trazo/Gaba 2.5/25 mg, − 3 for Trazo/Gaba 5/50 mg, and – 3.5 for Trazo/Gaba 10/100 mg, with a two-tailed confidence level of 95% a power > 85%, assuming a standard deviation of 2.3 and 20% of withdrawals. Forty patients were also added for the Gaba group for assay sensitivity, reaching a total sample size of 240 patients.
For statistical purposes, the safety population was defined as all randomized patients who took at least one dose of the study medication, while the m-ITT population was defined as all randomized patients who took at least one dose of the study medication and having a baseline and at least one post-baseline NRS evaluation. The LOCF method was implemented as imputation scheme for missing data in the m-ITT population.
The primary efficacy endpoint between Trazo/Gaba and PLB was evaluated in the m-ITT with LOCF, using an analysis of covariance (ANCOVA), including treatment and centers as factors and baseline as covariate and applying linear contrast test, excluding the active treatment (Gaba). Only if the linear contrast test was significant (p < 0.05), would the step-down Dunnett test be used to determine the minimum effective dose significantly different from PLB. If linearity was not verified (p > 0.05), an ANCOVA model, including treatment and center as factors and baseline as covariate, and comparisons with Dunnett test would be performed for the primary endpoint in the LOCF m-ITT and PP populations. If statistical assumptions underlying the ANCOVA were not satisfied, an ANOVA model would be applied. Before the application of the ANCOVA model, the non-significance of interaction treatment per baseline was verified.
Furthermore, mixed models for repeated measures (MMRM) in the m-ITT population were conducted as supportive analysis on the primary endpoint.
All secondary efficacy endpoints were reported descriptively in the m-ITT population. An ANCOVA or Cochran–Mantel–Haenszel test was applied, if appropriate. All secondary endpoints and secondary analyses were of exploratory nature and therefore no adjustment for multiplicity was planned.
Comments (0)