
Remember me

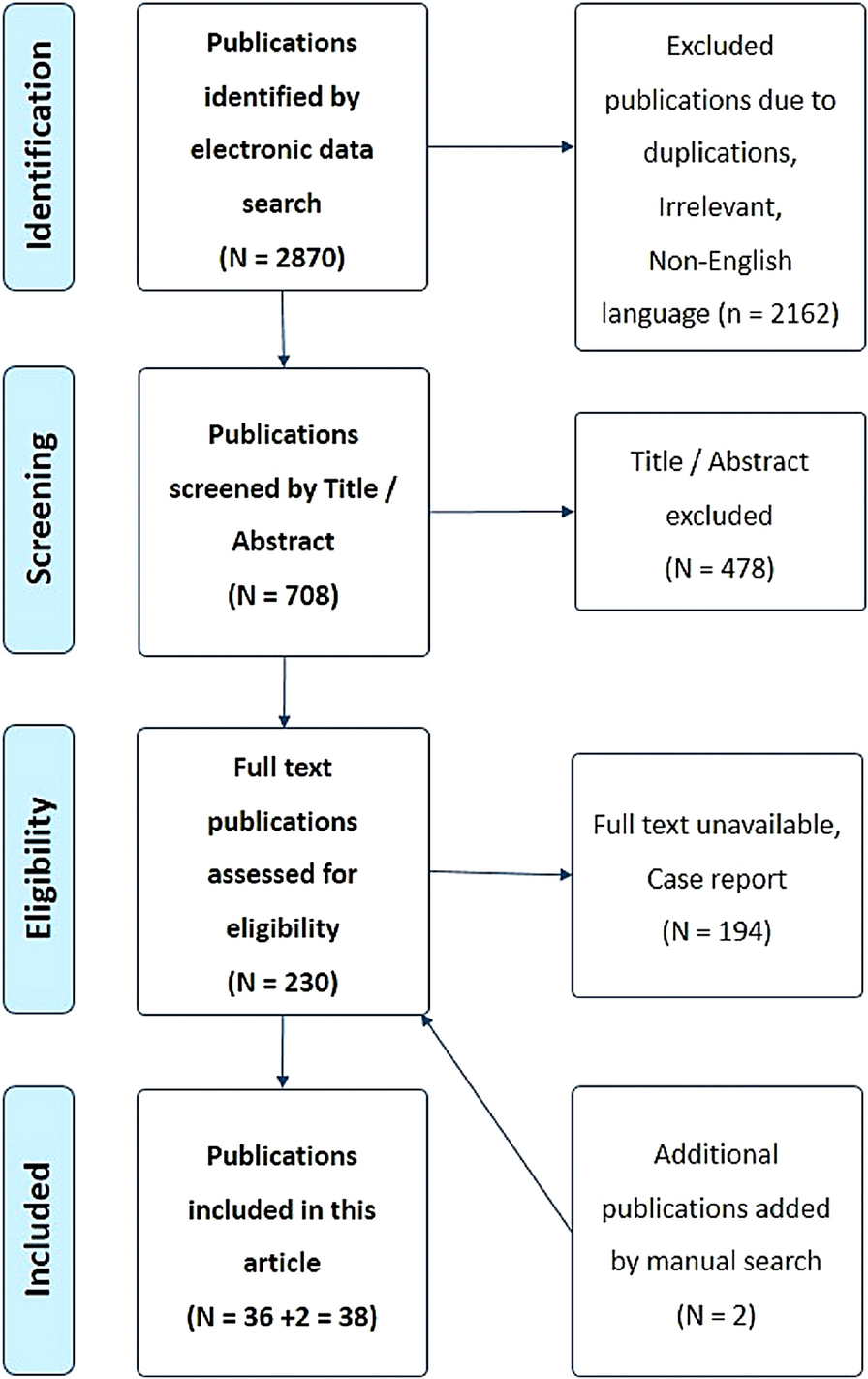
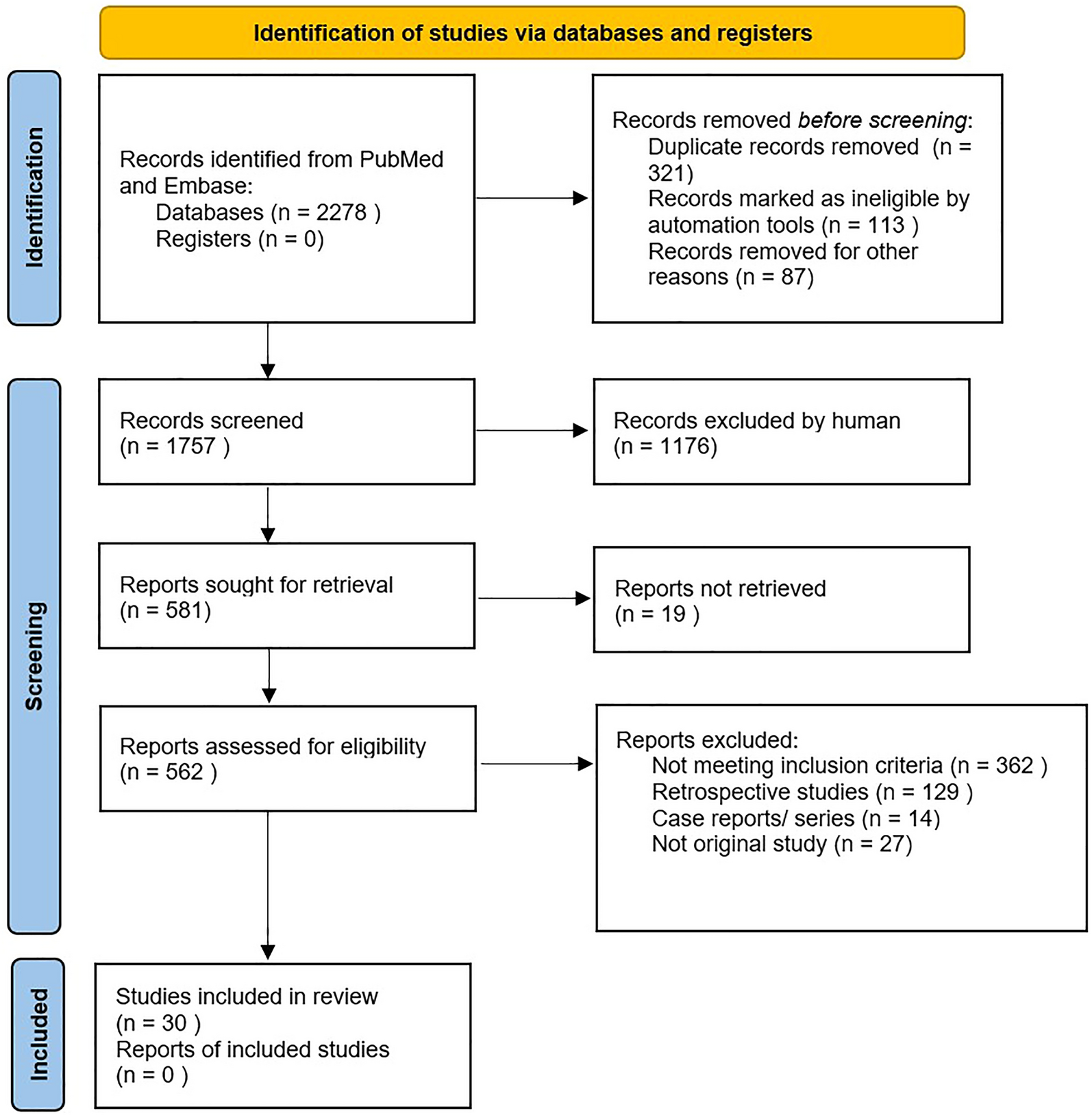
In total, n = 3138 results (Fig. 2) were found in the primary literature search. After screening based on title and abstract, n = 252 studies were qualified. After reviewing the full text, n = 42 studies were evaluated according to the Jadad scale and scientific validity, and studies were comprehensively analyzed. Results of the evaluation can be found in Supplementary Table 2–4. A summary and analysis of all studies are depicted in Table 1 and in more detail in the supplementary material (Supplementary Table 5).
Fig. 2
Flowchart and results of systematic literature search. Extended and translated from Likar et al. 2023 with permission [40]
Table 1 Summary and analysis of studies of auricular vagus nerve stimulation (aVNS) in chronic pain, acute post-surgery pain and acute experimental pain (short version, details in Supplementary Table 5)The risk of bias was assessed in a total of n = 22 studies for chronic and acute pain (Table 2).
Table 2 Results of the risk-of-bias 2 tool assessment [46]Chronic PainTwenty-three studies on chronic pain with a total number of n = 696 (n = 725 including dropouts) aVNS-treated patients were included in the analysis. These studies addressed chronic inflammatory bowel disease/abdominal pain (7 studies [49,50,51,52,53,54, 70], n = 150), migraine (4 studies [36, 55,56,57], n = 134), back pain (6 studies [56, 58,59,60,61,62], n = 229), rheumatoid arthritis (RA)/osteoarthritis (2 studies [63, 64]; n = 45), fibromyalgia/systemic lupus erythematosus (SLE) (3 studies [65,66,67], n = 49), chemotherapy-induced peripheral neuropathy (1 study [68]; n = 58), nonspecific chronic pain (1 study [49], n = 3) and chronic pain with depression comorbidity (1 study [69], n = 28). Of these, 12 studies [36, 50, 51, 57,58,59,60, 62, 65, 66, 69, 70] were high-quality RCTs with an average score of 7.2 out of 9 (Supplementary Table 2). One study [53] was designed as a randomized cross-over study with a rating of 5 points. Furthermore, seven case series [49, 52, 54,55,56, 63, 64], two retrospective cohort studies [61, 68] and one case-control study [67] with an average score of 3.5 points were identified.
Pain on a VAS or NRS, psychological well-being and tolerability/safety of stimulation were the most common primary and secondary endpoints. Depending on the indication, (additional) more specific symptom-related and disease-relevant endpoints were chosen.
In most of the studies, an improvement on VAS or NRS pain scale or a more specific disease-related endpoint was observed, with this improvement being statistically significant in 18 studies compared to baseline and/or compared to the chosen control group (see Table 1). In 3 of the 12 RCTs (for chronic back pain and abdominal pain), sustained pain reduction over up to 12 months was documented [50, 58, 60].
In eight studies [52, 55, 57, 58, 60, 61, 63, 68], the demand for pain medication was assessed. In six of these studies (3 for chronic back pain, 1 for chronic migraine, 1 in chemotherapy-induced peripheral neuropathy, 1 in irritable bowel syndrome) [52, 57, 58, 60, 61, 68], pain medication intake was reduced during and/or after aVNS (compared to baseline and/or control group). Secondary outcomes such as psychological well-being, disability scores, anxiety, sleep, fatigue and quality of life also significantly improved in the majority of studies [50, 53,54,55, 57, 58, 60, 65,66,67, 69, 70].
Clinically and statistically highly significant results were shown for indications chronic low back pain [58], chronic cervical syndrome [60], myofascial pain syndrome (neck) [59], depression with chronic pain [69], chronic abdominal pain [50, 51, 70] and chronic migraine [36, 55, 57].
In the present studies, aVNS was most used concomitantly to drug therapy. The average treatment period was 5.7 (1–26) weeks. However, duration of treatment as well as stimulation parameters within these applications could differ remarkably.
In three studies [36, 55, 67], fMRI examinations were performed alongside therapy to characterize the influence of aVNS on brain activity. fMRI revealed particularly an increase in brain connectivity in the areas of the executive control network (prefrontal brain regions), thalamus and cerebellum during or shortly after aVNS.
Fourteen studies were included in the risk-of-bias analysis. Only one study was rated low risk of bias [50], three studies with some concern [36, 65, 69] and ten studies with an overall high risk of bias [51, 53, 57,58,59,60, 62, 66,
Comments (0)