
Remember me




Although just 13.8% of all US residents live in a rural county,1 they bear an unbalanced proportion of the cancer burden. They have significantly higher cancer incidence and death rates for many cancer types and all cancer types pooled together.2 Many rural residents diagnosed with cancer encounter challenges accessing treatment3 because of lower availabilities of oncologists in rural areas,4 longer travel times to cancer treatment centers,5,6 or difficulties coordinating care with local primary care professionals.7
Once cancer treatment ceases, cancer survivors need continued clinical care to monitor cancer recurrence, detect new cancers, and monitor for treatment side effects.8,9 The American Society of Clinical Oncology (ASCO),10 the National Comprehensive Cancer Network,11 and the American Cancer Society (ACS)12 have developed survivorship care guidelines, and adherence to survivorship recommendations has been shown to be positively associated with health outcomes.13 Discussions between survivors and healthcare professionals about survivors’ posttreatment needs are arguably a key step to assuring the receipt of recommended cancer services. Furthermore, survivors who discuss in detail with a healthcare provider their emotional or social needs are less likely to report symptoms of depression and more likely to report positive attitudes toward cancer.14
Rural cancer patients’ inequities persist when transitioning into the survivorship period, as they have worse health outcomes compared with survivors residing in urban areas.15 One nationally representative study found that greater proportions of rural cancer survivors have poorer self-rated health, greater psychological distress, and multiple noncancer comorbidities than urban survivors.15 A study conducted in Kentucky also found that rural survivors have poorer mental health than urban survivors.16 Compounding their poorer health outcomes, rural survivors nationally are more likely to experience financial adversity because of their cancer.17
Improved survivorship care could ameliorate rural versus urban disparities in cancer survivorship outcomes, but very little research has examined rural versus urban differences in discussions about survivorship care. One prior study based on the 2011 Medical Expenditure Panel Survey (MEPS) found no rural/urban difference in cancer survivors’ discussions with healthcare providers about the need for follow-up care,18 but this study did not investigate discussions of other dimensions of survivorship care, such as healthy lifestyle recommendations, emotional or social needs, side effects, or treatment summaries.
This study’s overall objective was to test for rural versus urban inequities in cancer survivors’ discussions of survivorship care needs with their health care professionals. Given prior research documenting that rural residents frequently encounter difficulties accessing cancer treatment,3 we hypothesized that rural cancer survivors would have lower odds of discussing in greater detail key components of survivorship care: the need for follow-up services after completing treatment, lifestyle and health recommendations, emotional/social needs, long-term side effects, and a summary of treatments received. A secondary objective was to identify other predisposing, enabling, and need factors associated with discussions about survivorship care.
METHODS Study Design and SampleThe study design is cross-sectional and involves analyses of data from the 2017 Medical Expenditure Panel Survey (MEPS), which is the latest MEPS to include a cancer survivor module.19,20 The MEPS is sponsored by the US Agency for Healthcare Research and Quality (AHRQ) and is the federal government’s most thorough nationally representative survey of health services access among the civilian, noninstitutionalized population.19 MEPS participants are sampled from the National Health Interview Survey (NHIS) participants and complete a series of interviews.20
This study used data from 2 MEPS sources: the MEPS Household Component and the MEPS Experiences with Cancer Survivorship cgqlement. The MEPS Household Component includes information on demographic, social, economic, health, and healthcare utilization characteristics. In 2011, 2016, and 2017, the MEPS also included the Experiences with Cancer Survivorship cgqlement, which was collaboratively developed by experts from the National Cancer Institute (NCI), ACS, Centers for Disease Control and Prevention (CDC), and AHRQ.20 A sample of adult cancer survivors participating in the MEPS completed a self-administered questionnaire that assessed cancer-related psychological and financial burdens, long-lasting effects of treatment and cancer itself, effects on the employment of both survivors and their families, and survivors’ experiences discussing with healthcare professionals their survivorship care needs. The unweighted sample size for the Cancer Survivorship Supplement is 718 and the weighted sample size is 19,541,149. For the analyses presented in this article, persons whose only type of cancer was nonmelanoma skin cancer were excluded from analysis. When excluding these cases, the unweighted sample size is 569 and the analytical weighted sample size is 14,934,093 (2,542,041 rural and 12,392,052 urban).
Conceptual FrameworkAndersen and Aday’s well-established Behavioral Model of Health Services21,22 was applied to examine how individual-level predisposing, enabling, and need factors were associated with discussions about survivorship care. The Behavioral Model has been applied in numerous studies of adult cancer survivors’ health services use23 and racial/ethnic disparities in adult cancer survivors’ delays in medical care.24 More broadly, it has been applied in multiple investigations of rural versus urban disparities in healthcare access and outcomes.25–28
Dependent VariablesFive separate items from the MEPS Cancer Survivorship Supplement serve as separate dependent variables. Participants were asked, “Since you were diagnosed, did any healthcare provider discuss with you….” the following:
The need for regular follow-up care and monitoring even after completing your treatment? Lifestyle or health recommendations such as diet, exercise, or quitting smoking? Your emotional or social needs related to your cancer, its treatment, or the lasting side effects of that treatment? Late or long-term side effects of treatment you may experience over time? A summary of all the cancer treatments you received?Response options to each of the above questions were: (1) discussed it with me in detail; (2) briefly discussed it with me; (3) did not discuss it at all; and (4) I don’t remember. We combined “did not discuss it at all” and “I don’t remember responses,” similar to a technique used in prior research.29 The rationale for this approach is that persons who definitively recall engaging in discussion with a provider are more likely to actually adhere to the provider’s survivorship care recommendations.
Independent VariablesUS Office of Management and Budget designations of nonmetropolitan and metropolitan counties served as rural and urban classifications, respectively.30 Because the publicly available MEPS dataset does not include a rural/urban variable, the authors obtained from AHRQ a restricted use dataset that was analyzed at the US Census Bureau Research Data Center (RDC) located at the investigators’ university. Other predisposing variables included the survivors’ age, gender, and race/ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, or non-Hispanic other). Enabling factors were marital status (never married, married, widowed, or divorced/separated), highest educational attainment (less than high school, high school, college, or graduate school/other), family income as a percentage of the federal poverty level (poor, or <100%; low, or 100% to 200%; middle, or 200% to 400%; and high, or ≥400%), health insurance coverage (any private insurance, only public insurance, or uninsured during the year), and whether the respondent had a usual source of healthcare. Need factors included the years since cancer treatment (currently in treatment or <1 y, 1–3 y, 3–5 y, 5–10 y, 10–20 y, or ≥20 y since treatment; never treated; and unknown) and the number of comorbid conditions (0–1, 2–3, or 4 or more). For each variable, values of “not ascertained,” “don’t know,” “inapplicable,” or “refused” were coded as missing.
AnalysisWe conducted t-tests and chi-square tests to compare continuous and categorical variables across rural/urban residence. We then conducted ordered logit regression analyses using ordinal-dependent variables (1 = discussed it with me in detail, 2 = briefly discussed it with me, and 3 = did not discuss it at all or I don’t remember). To provide a supplemental and simpler portrayal of the relationships, we also conducted logit regression analyses using binary dependent variables (discussed with me in detail/briefly discussed it with me vs. did not discuss it at all/don’t remember), an approach which was used in another study.18 We originally included cancer types/sites (breast, colon, melanoma, non-melanoma skin, prostate, and other cancer) as independent variables in the analyses, but removed them from the final models because variance inflation factors indicated excessive multicollinearity. The models reported in the article therefore exclude cancer types/sites. All analyses were conducted with SAS survey procedures (SAS Institute, Cary, NC) to yield weighted estimates adjusting for the MEPS sampling scheme.31
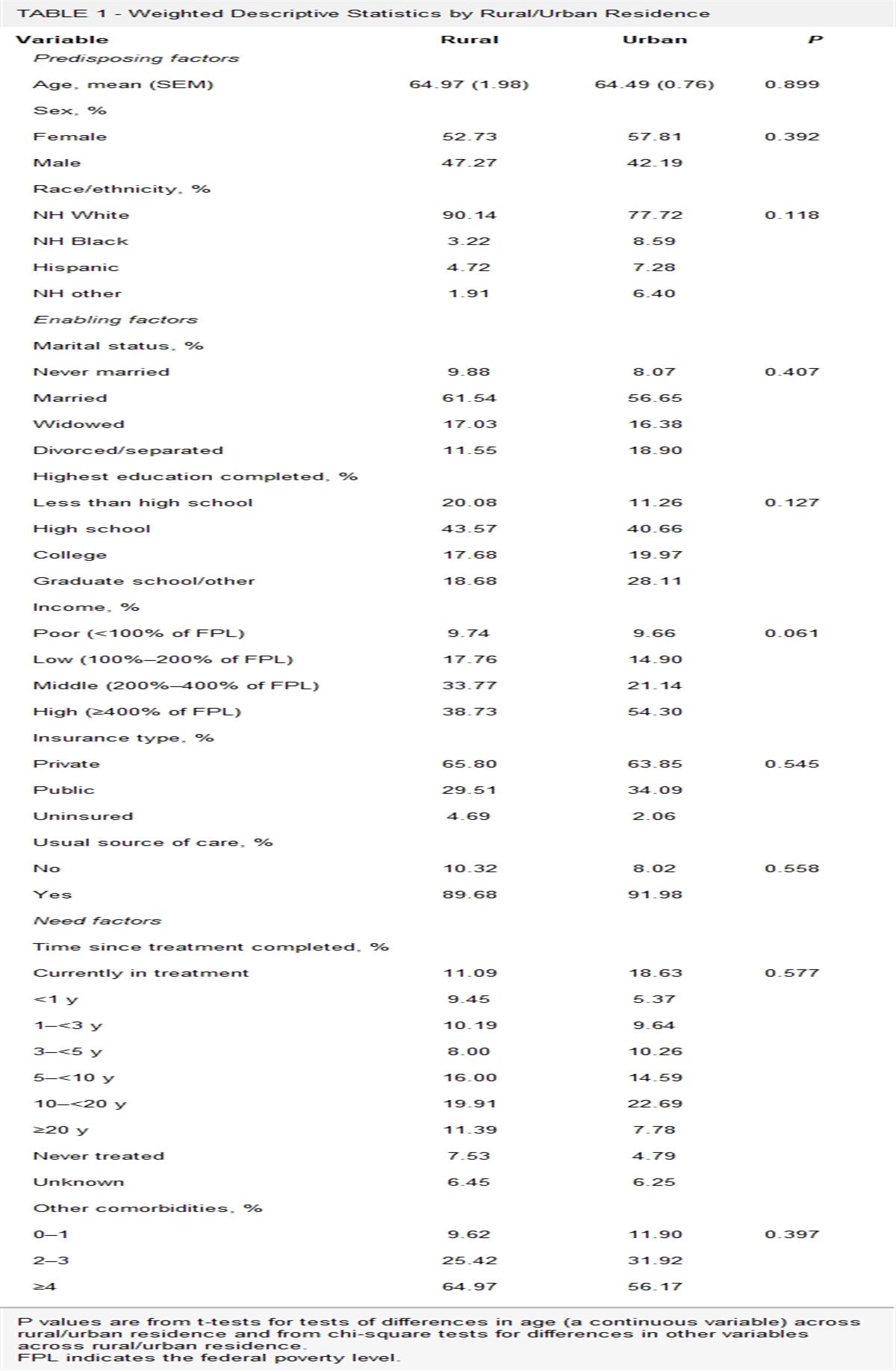
RESULTS Sample Characteristics by Rural/Urban ResidenceTable 1 shows that the sample characteristics did not differ significantly by rural/urban status. Regarding predisposing characteristics, both the rural and urban samples were ~64 years of age, had slightly higher percentages of females than males, and were predominantly non-Hispanic White. Regarding enabling factors, the majority of the rural and urban samples were married, well educated (only 20% of rural and 11% of urban had less than a high school degree), had middle or high incomes, and had a usual source of care. Regarding the need factors, the time since cancer treatment ended ranged from currently in treatment to more than 20 years since treatment, and the majority of rural and urban survivors had 4 or more comorbid conditions.
TABLE 1 - Weighted Descriptive Statistics by Rural/Urban Residence Variable Rural Urban P Predisposing factors Age, mean (SEM) 64.97 (1.98) 64.49 (0.76) 0.899 Sex, % Female 52.73 57.81 0.392 Male 47.27 42.19 Race/ethnicity, % NH White 90.14 77.72 0.118 NH Black 3.22 8.59 Hispanic 4.72 7.28 NH other 1.91 6.40 Enabling factors Marital status, % Never married 9.88 8.07 0.407 Married 61.54 56.65 Widowed 17.03 16.38 Divorced/separated 11.55 18.90 Highest education completed, % Less than high school 20.08 11.26 0.127 High school 43.57 40.66 College 17.68 19.97 Graduate school/other 18.68 28.11 Income, % Poor (<100% of FPL) 9.74 9.66 0.061 Low (100%–200% of FPL) 17.76 14.90 Middle (200%–400% of FPL) 33.77 21.14 High (≥400% of FPL) 38.73 54.30 Insurance type, % Private 65.80 63.85 0.545 Public 29.51 34.09 Uninsured 4.69 2.06 Usual source of care, % No 10.32 8.02 0.558 Yes 89.68 91.98 Need factors Time since treatment completed, % Currently in treatment 11.09 18.63 0.577 <1 y 9.45 5.37 1–<3 y 10.19 9.64 3–<5 y 8.00 10.26 5–<10 y 16.00 14.59 10–<20 y 19.91 22.69 ≥20 y 11.39 7.78 Never treated 7.53 4.79 Unknown 6.45 6.25 Other comorbidities, % 0–1 9.62 11.90 0.397 2–3 25.42 31.92 ≥4 64.97 56.17P values are from t-tests for tests of differences in age (a continuous variable) across rural/urban residence and from chi-square tests for differences in other variables across rural/urban residence.
FPL indicates the federal poverty level.
Table 2 shows that one of the 5 dimensions of survivorship care discussions differed significantly by urban/rural residence. Approximately 42% of rural survivors reported discussing treatments received in detail, compared to 52% of urban survivors (P=0.046). Approximately 69% of rural and 70% of urban survivors reported that they had discussed follow-up care needs in detail with a healthcare professional. Lower percentages discussed in detail with a healthcare professional lifestyle and health recommendations (36% rural, 43% urban), emotional/social needs (24% rural, 33% urban), and long-term side effects (44% rural, 50% urban).
TABLE 2 - Survivorship Care Discussions by Rural/Urban Residence Discussion Variable Response Rural (%) Urban (%) P Discussed follow-up care needs In detail 68.87 70.31 0.8961 Briefly 18.30 16.19 Did not/do not remember 12.83 13.50 Discussed lifestyle and health recommendations In detail 36.25 43.43 0.2828 Briefly 38.08 28.34 Did not/do not remember 25.67 28.22 Discussed emotional/social needs In detail 24.38 33.36 0.2045 Briefly 25.41 25.05 Did not/do not remember 50.22 41.59 Discussed long-term side effects In detail 43.54 49.88 0.502 Briefly 27.35 22.13 Did not/do not remember 29.10 27.98 Discussed treatments received In detail 42.26 52.29 0.046 Briefly 32.38 21.41 Did not/do not remember 25.36 26.29P values are from chi-square tests of differences in categorical discussion variables across rural/urban residences. Significant P values (<0.05) are bolded.
Table 3 shows findings from ordered logit regressions of discussions about follow-up care, lifestyle and health recommendations, and emotional/social needs. Table 4 shows findings from ordered logit regression analyses of discussions about side effects and treatments received. Significant odds ratios and corresponding 95% confidence intervals are bolded in the tables and significant P values are included in the text below.
TABLE 3 - Ordered Logit Regression Analyses of Discussions about Follow-Up Care–Lifestyle/Health Recommendations, and Emotional/Social Needs Follow-Up Care Lifestyle/Health Emotional/Social OR (95% CI) OR (95% CI) OR (95% CI) Predisposing factors Urban (vs. rural) 0.93 (0.55–1.58) 1.05 (0.60–1.82) 1.42 (0.90–2.22) Age 1.01 (0.98–1.03) 0.99 (0.97–1.01) 0.98 (0.97–1.00) Male (vs. female) 0.85 (0.55–1.31) 1.55 (1.03–2.33) 1.17 (0.81–1.69) Race/ethnicity (vs. non-Hispanic White) Hispanic 2.07 (0.72–5.95) 0.81 (0.39–1.70) 0.98 (0.44–2.21) Non-Hispanic Black 1.31 (0.61–2.80) 2.52 (1.22–5.20) 3.24 (1.68–6.26) Non-Hispanic other 1.12 (0.36–3.52) 2.33 (1.02–5.35) 1.94 (0.85–4.44) Enabling factors Marital status (vs. not married) Divorced/separated 1.11 (0.51–2.39) 1.33 (0.65–2.74) 1.20 (0.60–2.41) Married 1.08 (0.51–2.31) 1.60 (0.87–2.93) 1.96 (1.00–3.83) Widowed 0.60 (0.24–1.50) 0.50 (0.24–1.06) 0.88 (0.41–1.89) Education (vs. college) Graduate school or other 1.19 (0.60–2.37) 1.51 (0.86–2.67) 1.51 (0.86–2.68) High school 0.58 (0.31–1.08) 0.94 (0.59–1.51) 0.81 (0.47–1.41) Less than high school 0.42 (0.16–1.10) 0.75 (0.37–1.51) 0.77 (0.35–1.67) Income (vs. high) Poor 1.25 (0.56–2.79) 2.04 (0.94–4.43) 1.68 (0.84–3.38) Low 0.96 (0.54–1.73) 2.06 (1.07–3.98) 1.63 (0.92–2.88) Middle 1.59 (0.87–2.90) 1.76 (1.06–2.92) 1.41 (0.85–2.37) Insurance (vs. private) Public 0.73 (0.45–1.19) 0.77 (0.48–1.25) 1.19 (0.75–1.89) Uninsured 0.68 (0.19–2.41) 3.24 (0.96–10.94) 4.56 (1.71–12.16) Usual source of care (vs. none) 1.43 (0.66–3.07) 1.59 (0.82–3.07) 1.08 (0.55–2.11) Need factors Years since treatment (vs. in treatment) <1 y 1.49 (0.51–4.33) 1.56 (0.68–3.57) 0.5 (0.23–1.08) 1–<3 y 0.89 (0.35–2.22) 0.70 (0.33–1.46) 0.93 (0.46–1.91) 3–<5 y 1.97 (0.67–5.76) 0.46 (0.23–0.96) 0.25 (0.11–0.56) 5–<10 y 0.73 (0.32–1.67) 0.56 (0.32–0.97) 0.61 (0.34–1.09) 10–<20 y 0.69 (0.32–1.50) 0.55 (0.29–1.04) 0.48 (0.26–0.87) ≥20 y 0.43 (0.18–1.08) 0.38 (0.16–0.87) 0.47 (0.20–1.07) Never treated 0.46 (0.14–1.46) 0.24 (0.10–0.59) 0.19 (0.07–0.52) Unknown 0.29 (0.11–0.73) 0.45 (0.19–1.06) 0.47 (0.21–1.04) Other comorbidities (vs. 0–1) 2–3 0.91 (0.44–1.87) 1.02 (0.58–1.81) 1.19 (0.63–2.23) ≥4 0.91 (0.42–1.98) 1.10 (0.62–1.95) 1.47 (0.78–2.78)Dependent variable is coded as 1 = discussed in detail, 2 = discussed briefly, and 3 = did not discuss/do not remember. Significant (P<0.05) findings are bolded.
CI indicates confidence interval.
Comments (0)