
Remember me








Seventy-five patients participated in the HIGHSOX study. Among them, 43 patients were enrolled in this biomarker study and were measured baseline sHER2 ECD level. Patients` characteristic in this study are shown in Table 1. The median age was 64 years old, and around 80% of patients were male, ECOG PS0, stomach primary site, no previous gastrectomy, and HER2 IHC status 3 + . Almost 50% of patients had liver metastasis, and distant lymph node metastasis and peritoneal metastasis were found in more than 40% and 20% of patients, respectively. The median sum of the longest diameters of target lesions was 43 mm in this cohort. Patients` characteristic in this study was comparable to those of the HIGHSOX study [23].
Baseline HER2 ECD level and clinicopathological factorsDistribution of baseline sHER2 ECD levels is shown in Fig. 1a. The median baseline sHER2 ECD level was 12.8 ng/ml (Range 9.2–3440.0 ng/ml, Interquartile range; 11.1–19.1 ng/ml) with positivity rate of 39.5% in this study. Among clinicopathological characteristics, liver metastasis was significantly associated with higher baseline sHER2 ECD levels, while peritoneal metastasis was significantly associated with those of lower levels (Fig. 1b). No significant difference was shown in HER2 status (IHC3 vs IHC2 + /FISH +). In addition, a sum of the diameter in target lesions and baseline CEA levels showed significantly positive correlation with baseline sHER2 ECD levels. Multiple regression analysis including these factors showed that the sum of the diameter in target lesions was an only clinicopathological factor significantly related to baseline sHER2 ECD levels (Table 2).
Fig. 1
a Distributions of baseline serum HER2 ECD levels are shown. Normal values of serum HRE2 ECD were converted to base 10 logarithmic values. b Associations between patients’ characteristics and baseline serum HER2 ECD levels are shown. Several characteristics were significantly associated with baseline serum HER2 ESD levels, but HER2 status was not
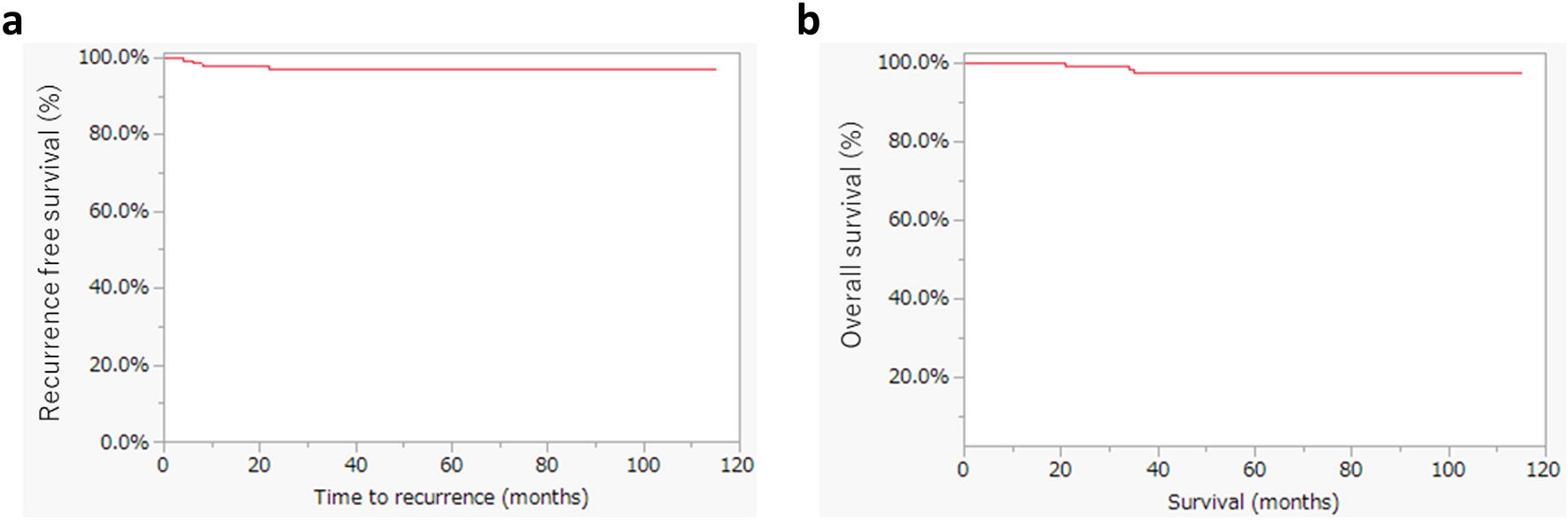
Table 2 Clinicopathological Features and Baseline Serum HER2 ECD LevelBaseline HER2 ECD level and treatment efficacyThe median follow-up period of all patients was 26.5 months, and the median follow-up period of censored patients was 79.3 months. The median PFS and OS of patients in this biomarker study was 11.3 months and 26.5 months, respectively, with ORR of 72.1%. These results were like those in the HIGHSOX study (Online Resource 1–3). Peritoneal metastasis and HER2 IHC2 + /FISH positive were chosen as a negative prognostic factor by univariate analysis in PFS. However, these factors did not remain after multivariate analysis. As for OS, stomach tumor, number of metastatic organs ≥ 2, distant lymph node metastasis and peritoneal metastasis were chosen as a negative prognostic factor by univariate analysis in OS. In multivariate analysis, distant lymph node metastasis and peritoneal metastasis remained as an independent negative prognostic factor for OS (Table 3).
Table 3 Patients' Characteristics and Prognostic Factors in This CohortThe quartile points of baseline sHER2 ECD levels were 11.1 ng/ml at the 25th percentile, 12.8 ng/ml at the 50th percentile, and 19.1 ng/ml at the 75th percentile, respectively. PFS and OS were compared by each quantile point of baseline sHER2 ECD levels, and there was a trend toward lower HRs for higher baseline sHER2 ECD levels both in PFS and OS (Fig. 2a). Because the hazard ratio point estimate was smallest at the 75th percentile of 19.1 ng/ml for both PFS and OS, the optimal cutoff for baseline sHER2 ECD levels was set at 19.1 ng/ml. When divided into two groups by baseline sHER2 ECD level of 19.1 ng/ml, mPFS and mOS was longer in the higher baseline sHER2 ECD group compared with the lower group (mPFS: 16.8 months vs 8.7 months, HR 0.70 95%CI 0.33–1.50, p = 0.359. mOS: 35.5 months vs 20.6 months, HR 0.64 95%CI 0.29–1.41, p = 0.270), respectively (Fig. 2b, c). As for the ORR, ORRs were comparable both in higher and lower groups even though divided by three selected cutoff values (Fig. 3).
Fig. 2
a Forrest plots show hazard ratios (HRs) by each quantile point of baseline serum HER2 ECD level. There was a trend toward lower HRs for higher baseline serum HER2 ECD levels both in PFS and OS, respectively. Kaplan–Meier curves of PFS b and OS c divided by baseline serum HER2 ECD with cutoff value of 19.1 ng/ml are shown, respectively
Fig. 3
Forrest plots show objective response rates (ORR) by each quantile point of baseline serum HER2 ECD level and its early change. ORRs were comparable both in higher and lower baseline serum HER2 ECD groups even though divided by three selected cutoff values, while higher ORRs were shown in higher reduced group
Early changes in HER2 ECD during treatment and treatment efficacyAmong 43 patients, 39 patients were measured sHER2 ECD at least once within 3 cycles other than before their initial treatment. After initiation of treatment, sHER2 ECD had significantly decreased up until the third cycle (Fig. 4). Given that sHER2 ECD correlated with the sum of tumor diameter in target lesions and the significant decline in sHER2 ECD observed in the early after treatment, we next investigated the potential surrogate role of early sHER2 ECD reduction in treatment response. The quartile points of early changes in sHER2 ECD were 12.9% at the 25th percentile, 29.5% at the 50th percentile, and 42.5% at the 75th percentile, respectively. PFS and OS were compared by each quantile point of early changes in sHER2 ECD, and there was also a trend toward lower HRs for higher reduction rates of sHER2 ECD both in PFS and OS (Fig. 5a). Since the hazard ratio point estimate was smallest at the 75th percentile of 42.5% for both PFS and OS, the optimal cutoff for early changes in sHER2 ECD was set at 42.5%. When divided into two groups by reduction rate of 42.5%, mPFS and mOS were longer in the higher reduced group compared with the lower group (mPFS: 17.2 months vs 8.7 months, HR 0.49 95% CI 0.21–1.13, p = 0.095. mOS: 65.0 months vs 17.8 months, HR 0.40 95% CI 0.16–0.99, p = 0.047), respectively (Fig. 5b, c). As for the ORR, similar trends were shown when divided into two groups by reduction rates of 29.5% and 42.5%, ORRs were higher in the higher reduced group compared with the lower group (90% vs 63.2% for 29.5%, p = 0.065. 100% vs 70% for 42.5%, p = 0.085), respectively (Fig. 3).
Fig. 4
Changes in serum HER2 ECD during treatment are shown. After initiation of treatment, serum HER2 ECD had significantly decreased up until the 3rd cycle
Fig. 5
a Forrest plots show hazard ratios (HRs) by each quantile point of early changes in serum HER2 ECD level. There was a trend toward lower HRs for higher reduction rates of serum HER2 ECD both in PFS and OS, respectively. Kaplan–Meier curves of PFS b and OS c divided by reduction of 42.5% are shown, respectively. Patients who achieved a reduction rate of ≥ 42.5% within the first three treatment courses were significantly associated with longer OS
Among 39 patients, 9 patients achieved the reduction rate ≥ 42.5% up until the third treatment courses. Among those 9 patients who achieved the reduction rate ≥ 42.5%, baseline sHER2 ECD levels were positive in 7 patients (77.8%) (Table 4). Whereas, among 30 patients who did not achieve the reduction rate ≥ 42.5%, baseline sHER2 ECD levels were negative in 22 patients (73.3%) (p = 0.015). Moreover, in nine patients who achieved this reduction rate up until the third treatment courses, 7 patients measured sHER2 ECD at the second cycle. Importantly, 6 out of 7 patients (85.7%) achieved the reduction rate ≥ 42.5% at the second cycle (3 weeks).
Table 4 Baseline sHER2 ECD positivity and achievement of reduction rate ≥ 42.5%
Comments (0)