
Remember me






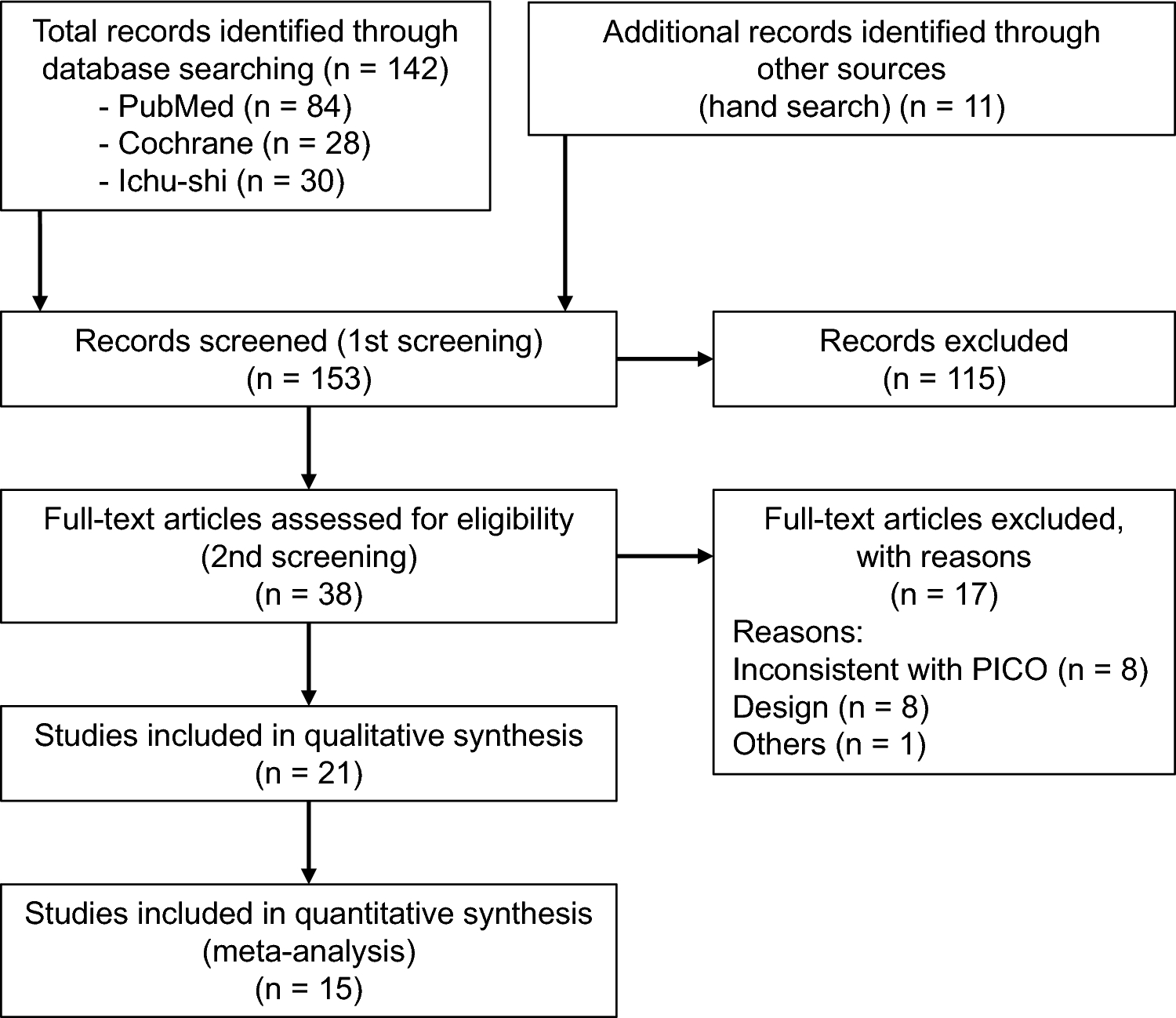


Among 1791 mBC patients with abstracted data, 312 had HER2 + tumors and received 2 or more lines of therapy in the metastatic setting (Fig. 1). Median follow-up for all patients was 22 months (IQR, 13–37) from the index date. Median age at mBC diagnosis was 57 (IQR, 49, 64) years. The majority of patients were white (69%), non-Hispanic (86%), resided in the Midwest (89%), and were diagnosed with de novo metastatic disease (62%) (Table 1). At the start of 2L, 54% were hormone-receptor positive and 34% of patients were “triple positive” for ER, PR, and HER2. Over half of patients (56%) were postmenopausal at initial diagnosis. The Black or African American population (21%) had a median age of 53 years [IQR, 45–63] at mBC diagnosis (median age White: 57 years [IQR, 49–64]) and 55 years [IQR, 46–55] at 2L initiation (median age White: 59 years [IQR, 51–66]); more than two-thirds (69%) were diagnosed with metastatic disease at initial diagnosis (White: 62%). Patients in the T-based 2L subcohort (n = 116) had similar characteristics and are included in Table 1 with a median follow-up of 16 months (IQR, 16–45).
Fig. 1
CONSORT diagram for the study cohort detailing criteria applied to reach the final sample of patients with 2 or more lines of therapy in the metastatic setting
Table 1 Demographic and clinical characteristics of included patientsTreatment characteristicsPre-metastasis treatmentOf 312 patients, 114 were diagnosed with recurrent metastatic disease (Supplementary Table S1). Nearly all (107/114, 94%) received surgery for removal of primary disease; 75% were mastectomies. Half received neoadjuvant treatment of any kind (59/114), of which 73% (43/59) received a HER2-targeted therapy. In the adjuvant setting, 75% (85/114) received any treatment; and 51% of those receiving treatment (43/85) received a HER2-targeted agent. Approximately two-thirds of all 312 patients (63%) received radiation to the primary site. Similar proportions were observed in the T-based 2L subcohort. However, within the T-based 2L subcohort only 60% (12/20) of patients with neoadjuvant treatment and 38% (13/34) of patients with adjuvant treatment received HER2-targeted therapies.
Systemic treatment in the metastatic settingMore than half of the 312 patients (54%) initiated 2L therapy from 2018 and onwards; 37% received only 2 LoTs, 29% only 3 LoTs, and 35% received ≥ 4 LoTs. A similar distribution was observed in the T-based 2L subcohort.
In 1L, 87% of all patients and 82% of the T-based 2L subcohort received a HER2-targeted therapy, either as monotherapy or in combination with other agents (Fig. 2). Most patients received a T-based regimen (All patients: 78%; T-based 2L subcohort: 68%). Among all patients, the three most frequent regimens in 1L were trastuzumab + pertuzumab + taxane (40%); trastuzumab + pertuzumab + taxane + carboplatin (11%); and trastuzumab monotherapy (10%). Half of patients (52%) received 1L standard-of-care treatment consisting of taxane + trastuzumab + pertuzumab (THP) with or without other agents. The most common regimens in 1L for the T-based 2L subcohort were trastuzumab + pertuzumab + taxane (28%); trastuzumab (14%); T-DM1 (9%). In 1L, 7% patients received T-DM1; 15/51 in the HER2-targeted monotherapy group and 7/222 in the HER2-targeted combination group.
Fig. 2
Distribution of First (1L), Second (2L), and Third-Line (3L) Regimen among all patients who received at least 2 lines of therapy in the metastatic setting (a) and patients who received a trastuzumab-based 2L regimen (T-based subcohort) (b). HER2-targeted regimen(s) include trastuzumab or a trastuzumab biosimilar, pertuzumab, lapatinib, margetuximab, neratinib, tucatinib or pyrotinib and the antibody drug conjugates (ADC) T-DM1 and T-DXd; chemotherapy-based regimens do not include HER2-targeted therapy; and other targeted therapy-based regimens do not include HER2-targeted therapy or chemotherapy. ADCs may be given as monotherapy or in combination with other antineoplastic therapies. “No treatment” includes patients who were on a 2L regimen at the end of follow-up and patients with no further documented treatment for any reason, including death and loss to follow-up
Among all 312 patients, 89% received HER2-targeted therapy in 2L, of which 42% received a T-DM1-containing regimen and 37% a T-based regimen (Fig. 2). The most common regimens were T-DM1 with or without endocrine therapy (29%), trastuzumab + pertuzumab + taxane (10%), and T-DM1 + trastuzumab (8%). In 2L, 20% (64/312) received standard-of-care T-DM1 monotherapy; however, an additional 22% (68/312) of patients received T-DM1 concurrent with another therapy. In the T-based 2L subcohort, the most common regimens were trastuzumab + pertuzumab + taxane (28%); trastuzumab + pertuzumab (11%); and trastuzumab + lapatinib (6%) in 2L. ADC-based regimens were given to 43% of patients in 2L; 65/103 in the HER2-targeted monotherapy group and 65/175 in the HER2-targeted combination group.
Subsequently, 63% [197/312] of patients received 3L and most continued to receive HER2-targeted regimens (all patients, 84% [166/197]; T-based subcohort, 86% [65/75]) (Fig. 2). The majority of patients received a T-based regimen (41%; 80/197) or a T-DM1-containing regimen (23%; 46/197) in 3L. In the T-based subcohort, patients were more likely to receive a T-DM1-based regimen (44%; 33/75) or a T-based regimen (39%; 29/75) in 3L. The most common regimens in 3L were T-DM1 (19%), T-DXd (10%), and capecitabine + lapatinib (8%) among all patients and T-DM1 (35%), T-DM1 + trastuzumab (7%), palbociclib (4%) in the T-based subcohort. Among patients who received HER2-targeted monotherapy, 45/61 received an ADC, while 23/105 patients who received a HER2-targeted combination regimen did.
2L reasons for discontinuationOnly 12% of patients from the full cohort and 18% in the T-based 2L subcohort remained on 2L at the end of follow-up. The majority of patients discontinued 2L (All patients, 88%; T-based 2L subcohort, 82%). Of the 274 patients who discontinued 2L in the full group, 20% died either while on 2L or after completing 2L treatment; 21 (8%) did not receive further treatment; and 72% started a new line of therapy. Similar patterns were observed in the T-based 2L subcohort (Table 2). In the full group, the three most common reasons for discontinuing 2L treatment were progression/worsening of cancer (47%); intolerance or toxicity with no evidence of progression (17%); and end of planned therapy (9%). The T-based 2L group discontinued 2L for the same top three reasons; however, the proportion of patients who completed planned therapy was 20% (Table 2).
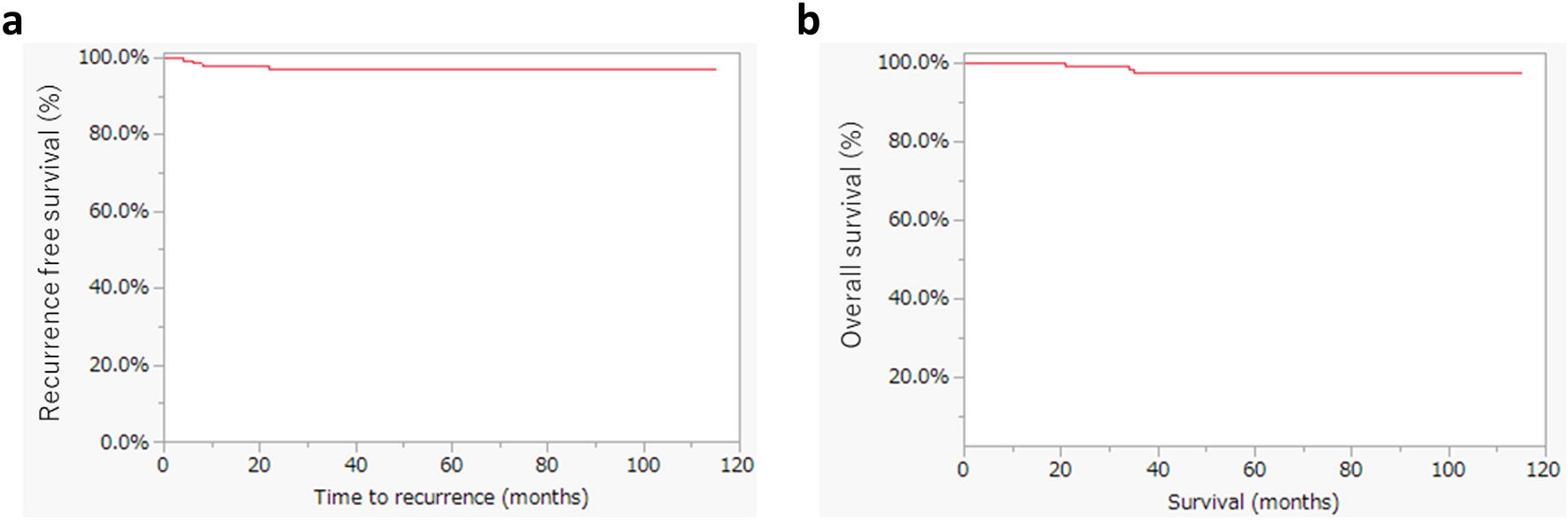
Table 2 Second-line (2L) treatment attrition and reasons for discontinuation2L-associated clinical outcomesFigure 3 summarizes clinical outcomes for all patients from the date of 2L initiation. The median TTD was 7.2 months (95% CI, 6.5–8.9). Median TTNT was 10.6 months (95% CI, 8.8–13.3); and median rwPFS was 7.9 months (95% CI, 7.0–9.9). Among 116 patients who received a T-based regimen in 2L, the median TTD was 10.6 months (95% CI, 7.4–14.0); median TTNT was 14.9 months (95% CI, 9.9, 22.0); and the median rwPFS was 13.6 months (95% CI, 8.3, 20.2).
Fig. 3
Clinical Outcomes for Second-Line Treatments in HER2 + mBC and median number of months-to-event from 2L initiation (index). a Time to treatment discontinuation (TTD) is the time from index to the first of treatment discontinuation or death; patients without the event were censored at the date of last contact or data cut-off (DCO), whichever came first. b Time to next treatment (TTNT) is the time from index to the first of 3L initiation or death; patients were censored the date of last contact or DCO, whichever came first. c real-world Progression-free survival (rwPFS) is the time from index to the first of clinician-confirmed progression or death; patients were censored at 3L initiation, last contact or DCO, whichever came first
Comments (0)