Neuromyelitis optica spectrum disorder (NMOSD) is an uncommon but severe inflammatory demyelinating condition that relapses and is presenting with catastrophic optic neuritis (ON). Vision impairment results from the optic neuritis in NMOSD, which damages the optic nerve and retina's neuroaxonal structure [32].
Vascular alterations are becoming more widely acknowledged as significant aspects in the pathogenesis of neuroinflammatory diseases, particularly neuromyelitis optica spectrum disorder (NMOSD), in addition to established immune-mediated processes [19].
Optical coherence tomography angiography (OCTA), a relatively new technology, provides depth-resolved, non-invasive pictures of the retinal and choroidal vasculature. OCTA measures vascular density rather than structural atrophy, offering a different quantitative indicator of retinal affection [19].
In this study, we aimed to assess the retinal vascular abnormalities through OCT angiography in NMOSD patients with or without a history of ON compared to each other and with healthy controls and investigate their correlations with neuroaxonal structural damage evaluated with spectral domain OCT (SD-OCT), as well as visual acuity (VA) and other clinical outcomes.
Our results in this study found that NMOSD + ON patients had a statistically significant reduction in all SD-OCT parameters compared to healthy control but not in NMOSD–ON. With regard to OCTA, there was a significant reduction in radial peripapillary capillary density (RPCD) in NMOSD + ON in all sectors and some sectors of NMOSD–ON compared to healthy control. NMOSD + ON patients had significant differences in RPCD compared to those without history of ON. In NMOSD + ON patients, significantly positive correlation existed between all OCT and OCTA parameters and a negative correlation of both with visual acuity. Retinal microvascular changes were present in NMOSD–ON eyes indicating that subclinical primary retinal vasculopathy may occur in NMOSD prior to ON and RNFL atrophy.
These results goes with results of other studies as we will discuss in details and they give us an image about understanding the pathophysiology of NMOSD, and how it is changed from being only inflammatory disease to another pathology related to retinal vascular alterations which is also related to aquaporin-4 antibodies. these results will help us in early detecting cases with retinal affection even before development of ON attacks and structural damage allowing close monitoring to those patients and also as prognostic marker and also can be monitoring biomarker by serial follow-up retinal imaging by OCTA and detecting the changes and finally all this will reflected on disease management regarding early intervention with suitable DMTs, escalation during follow-up or finally for future medications that targeting this pathophysiology of the disease but this needs more research in this context.
The retinal microvasculature is an early and frequent target of inflammatory attacks in NMOSD. Changes in the retinal microvasculature in NMOSD patients are thought to be a sign of retinopathy onset and development [17]. Previous investigations support the concept that NMOSD is a primary astrocytopathy. In the retina, there exist AQP4 expressing astrocytic cells called ‘Müller cells’, which may be directly targeted by AQP4-ab and become a probable cause of primary retinopathy in NMOSD [33].
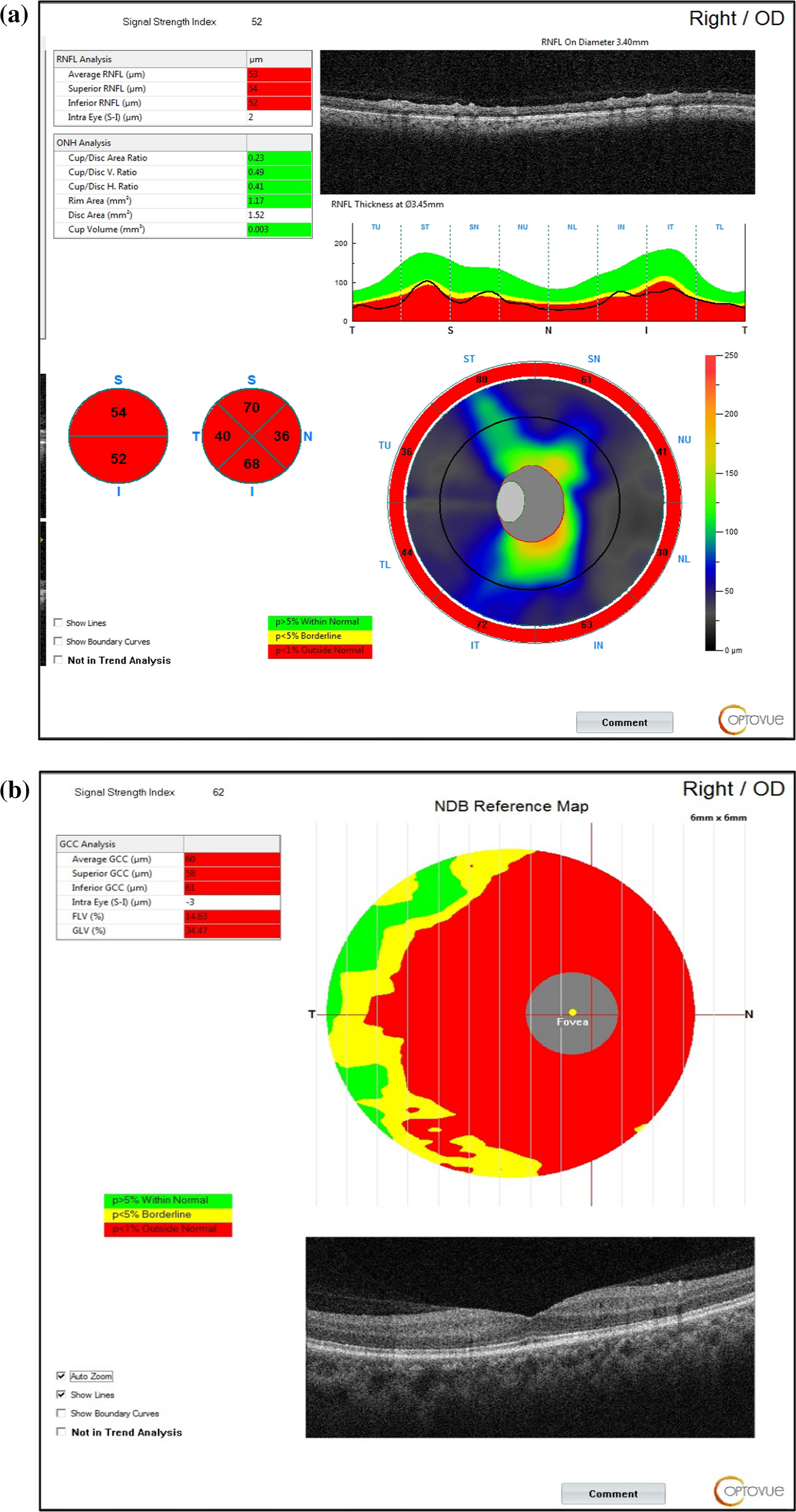
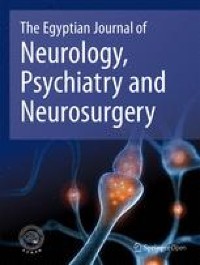
This study confirmed the presence of significant alterations in the retinal structure and microvasculature network in NMOSD patients with a history of ON, as compared to controls and patients without ON, all RNFL and GCC values were significantly lower in patients with ON, with a significant increase in focal and global loss volume (FLV, GLV) this implying severe structural and axonal degeneration but no significant difference in these parameters between patients without history of ON and healthy control. Similarly, RNFL and GCC thickness parameters were thinner in NMOSD + ON compared to healthy controls and NMOSD − ON and same results obtained by previous studies [16, 17, 33, 34] regarding SD-OCT parameters in NMOSD + ON and NMOSD–ON.
Also, in the NMOSD + ON group, a significant correlation was found between all SD-OCT parameters when correlated with visual acuity affection, denoting that the structural atrophy and volume loss of retinal layers strongly affect visual acuity. These findings agree with another study of Kwapong and colleagues [16] who found a significantly reduced structural thickness and microvasculature, as well as the association between these changes and impaired visual acuity.
This study demonstrated that there was no significant correlation between SD OCT parameters (RNFL, GCC thickness) and number of optic neuritis attacks in NMOSD + ON group.
Oertel and colleagues in 2021 found that first optic neuritis attack is usually severe than subsequent attacks, they explained these finding by longer time until reaching to effective anti-inflammatory therapy and the typical choice of less effective therapies (like steroids instead of plasma exchange) at the first attack compared with the following attacks. And the net results is more damage in first attack and reduced neuroaxonal content.
In agreement with previous studies [16, 17, 26], this study confirmed the presence of substantial alterations in the retinal microvasculature network in patients with NMOSD with or without a history of ON. This study revealed a significant reduction in vascular density in RPCD (whole image and all peripapillary grid sectors) in NMOSD + ON in comparison to healthy control. Also, there was a significant reduction in some RPCD sectors in NMOSD–ON compared to healthy controls.
Concurrently, this study revealed a significant difference in RPCD between NMOSD + ON and NMOSD–ON. Despite that, OCTA finding in NMOSD–ON compared to healthy control was not associated with any changes in SD-OCT parameters, which implies that vascular alterations occurred in NMOSD eyes even before the onset of ON and the occurrence of structural damage in the retina, denoting subclinical primary retinal vasculopathy.
Regarding the explanation of reduced retinal vascular density in NMOSD patients, according to Chen and colleagues [26], a pathological study of NMOSD patients revealed that the vascular walls of the optic nerve were penetrated by inflammatory cells. Damaged astrocyte and vascular endothelial cells that induced by inflammation likely directly reduces vascular perfusion and could facilitate neurodegeneration. Müller cells are responsible for water homeostasis, energy metabolism, and neurotransmitter recycling, and maintaining the function of the blood–brain barrier. High level of aquaporin-4 are expressed by these retinal astrocytic cells. Thus, Müller cells may likely be attacked by AQP4-ab before the occurrence of ON, causing retinal vascular rarefaction in patients with NMOSD [26, 33]. This suggests that NMOSD has subclinical disease activity and might drive relapse-independent disease progression [25].
Consistent with previous studies [16, 17, 35], this study showed a significantly negative correlation between all RPCD parameters and visual acuity impairment in NMOSD patients with ON. Also, there is a significant negative correlation between number of ON attacks and vessel density in RPCD, proving that the increased frequency of ON worsen the microvascular impairment in NMOSD. This goes with the results of Kwapongand colleagues [35]. In contrast, Huang and colleagues [17] found no significant correlations between vessel density parameters and the number of ON attacks. This may explain why this current study involved more sectors in OCTA than Huang’s study (13 sectors in this current study versus seven sectors in his study in RPCD). This study goes in agreement with other studies of Huang and colleagues [17], Kwapongand colleagues[16], who found that in NMOSD + ON patients, the peripapillary vessel densities correlated well with the spectral domain OCT parameters (RNFL, GCC), suggesting that the vascular alterations are related to structural damages involving the retina and both related to poor visual outcome.
This study found a significant positive correlation between some OCT parameters (RNFL, GCC) and RPCD in NMOSD-ON. This goes with Huang and colleagues [17] who found a correlation between RPCD and OCT parameters, indicating that these subclinical changes may be interconnected to a certain degree.
Multivariate logistic regression analysis in this study found that peripapillary capillary density, especially the nasal inferior sector, is the most accurate predictor for detecting subclinical optic nerve affection in the NMOSD–ON group between all OCT and OCTA parameters.
RPCD is only vascular plexus in OCTA correlated with SD OCT parameters in NMOSD – ON group. In comparing NMOSD + ON and NMOSD – ON groups, there was highly significant difference between them in RPCD, which means that involvement of RPCD is marked in NMOSD + ON compared to NMOSD – ON.
These results goes in agreement of Huang and his colleagues 2019 that patients with poorer peripapillary perfusion may present with more severe visual acuity impairment and that peripapillary vessel density may be a surrogate predictor of visual outcomes in NMOSD patients with ON.
From these previous points, we can conclude that RPCD is the earliest vascular plexus to be affected in NMOSD – ON group and also the most severely affected plexus in NMOSD + ON group. The identified biomarkers and observed alterations may contribute to the early diagnosis and monitoring of NMOSD, potentially offering a time window for intervention and prevention of disease progression [36,37,38].
This study had some limitations. First, a small sample size prevented a more comprehensive comparison study between NMOSD patients subgroups (NMOSD with ON versus NMOSD without ON) as NMOSD-ON group was much lower. A larger sample size is needed to prove the results regarding OCT and OCTA. Second, its cross-sectional design made it impossible to determine the exact sequence of the medical events; we cannot demonstrate whether vascular alterations are secondary to fewer energy requirements from the atrophied retina or a primary process causing generalized ischemia with secondary retina atrophy. Therefore, longitudinal studies are necessary to support this hypothesis about microvascular alterations. Also, the broad age spectrum in this study (15–50) is considered a weak point, as we are comparing extremely different ages in their retinal vascular changes. Age may be a corresponding factor in these changes.

留言 (0)