
記住我







This secondary analysis was part of a clinical trial which was performed as a prospective, single-center, randomized controlled clinical trial (see CONSORT checklist). The effects of an intensive oral prophylaxis program (= OPP) were compared with standard statutory health insurance prophylaxis (treatment as usual = TAU) on halitosis among young patients with renal insufficiency. OPP included instructions related to tongue cleaning, among others. The trial was approved by the Ethics Committee of the Faculty of Medicine at the University Hospital of Cologne (#15–264) and recorded at The German Clinical Trials Register (#DRKS00010580).
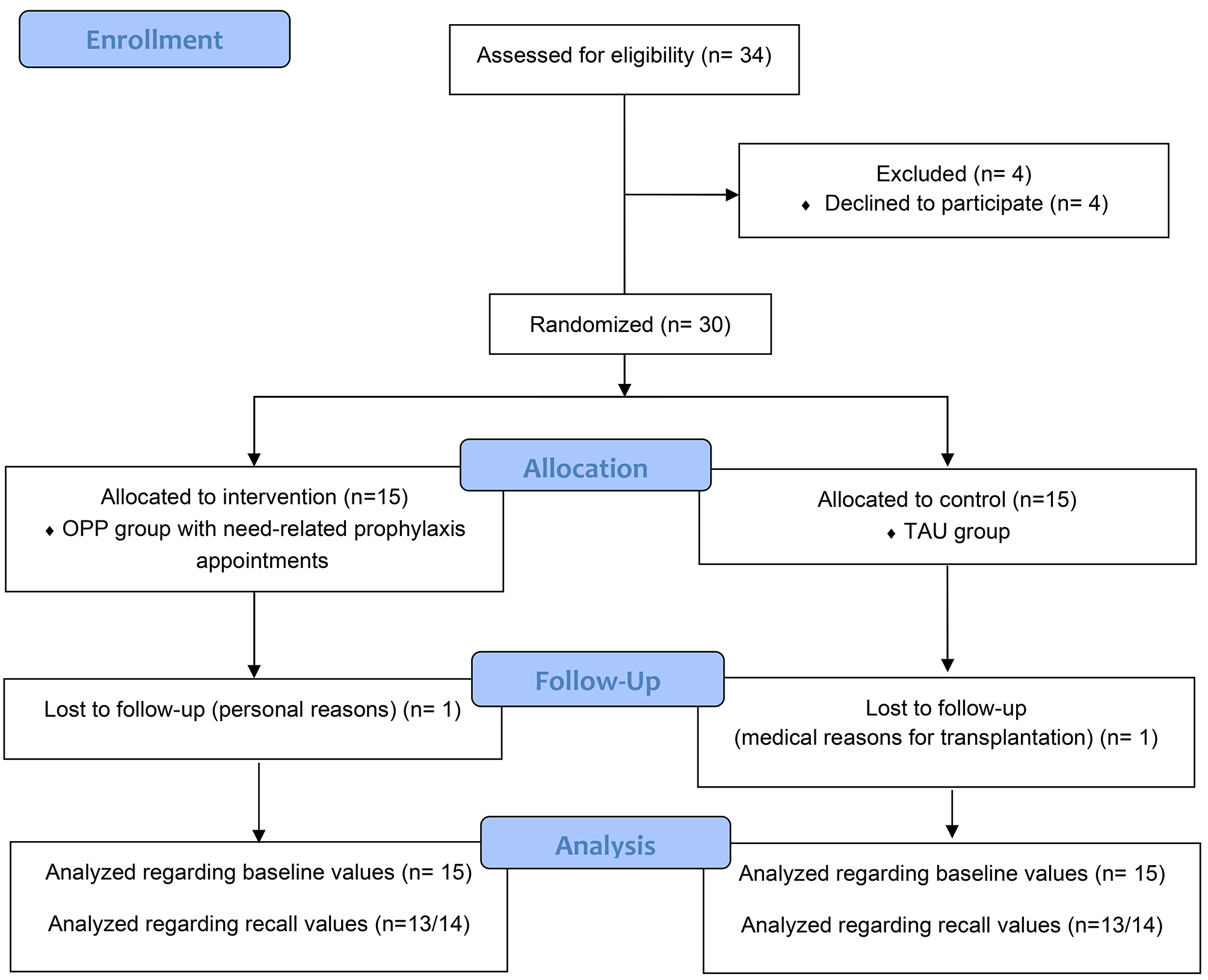
Patient recruitment and randomizationPatients were initially screened for study enrollment by pediatric nephrologists and then pediatric dentists, and randomly assigned to the intervention or control group via a computer-guided program, TENALEA (ALEA, Abcoude, NL). Patients attending the Department of Pediatric Nephrology at the University Hospital who fulfilled the following inclusion criteria were enrolled in the study: patients with CKD grade 1–5 according to the ‘Kidney Disease: Improving Global Outcomes’- (KDIGO)- classification [criteria for advanced CKD according to the glomerular filtration rate and albuminuria [16]], patients undergoing conservative treatment, and those already transplanted or dialyzed; patients with gingivitis. Any signs of acute infection and/or fever or antibiotic treatment in the 14 days prior to participation were defined as exclusion criteria. This decision was made by the treating pediatric nephrologists based on clinical parameters and blood tests. Figure 1 shows the CONSORT flow chart and Fig. 2 highlights the timeline of this study.
Fig. 1 Fig. 2
Fig. 2 Study measures
Study measuresThe main parameters studied were the VSCs HS, DMS and MM, measured by gas chromatography (OralChroma™ CHM-1) and the Winkel Tongue Coating Index [15] as well as the Quigley Hein Index (QHI) and the Papillary Bleeding Index (PBI) at three time points: baseline, 3 months after dental prophylaxis, 6 months after baseline. At baseline, an intraoral dental examination, including dmft/DMFT caries diagnostics (according to the International Caries Detection and Assessment System) was performed. Caries restorative measures were carried out when needed. The focus of this paper lies on the halitosis-related measurements such as VSCs and Winkel Index. OralChroma uses an indium oxide semiconductor gas sensor; it does not require a carrier gas like conventional gas chromatographs, but instead uses room air as a carrier for the chromatography column. To ensure the validation of VSC measurements, the OralChroma device was calibrated by the manufacturers (Abilit Corporation, Japan) before the study began according to their guidelines. OralChroma has been described as one of the most appropriate methods to detect halitosis of different origins (intra- and extra-oral halitosis) [17]. Patients were instructed to refrain from foods containing garlic, onion and spices 24 h prior to measurements. Furthermore, tooth brushing, mouth rinsing or chewing gum were only permitted up to 1 h prior to measurements. All measurements were supposed to take place in the mornings and were carried out by the same examiners (KH and IG). For sample collection, a disposable syringe (0.5 mL) was inserted two-thirds into the patient’s oral cavity for 30 s. The plunger was slowly pulled out and pushed back in twice more, before the definitive sample was taken and injected into the analyzer. After processing was completed, the concentration of VSC was visualized in parts per billion (ppb) by the OralChroma Data Manager software package. As the cognitive threshold values are reported differently in the literature, relevant limits of detection were chosen as 95 ppb for HS, 12 ppb for MM and 24 ppb for DMS, in accordance with Tangermann und Winkel [18].
In addition, the Tongue Coating Index according to Winkel was measured. For this Winkel Index, the tongue was imaginarily divided in six areas- three anterior and three posterior parts. Tongue coating was then scored as 0 = no coating, 1 = light coating or 2 = severe coating; in general, a score between 0 and 12 is the result [13].
Furthermore, short, narrative interviews were conducted with all patients and their mothers mainly regarding self-perceived oral malodor in the course of an extended anamnesis in order to determine potential impairments due to possible halitosis. In addition, five nurses were asked about their perceptions of halitosis in young CKD patients during study-related visits at the CKD unit. Quotes from these discussions were recorded verbatim. The qualitative content analysis was performed by two experienced researchers (KH and IG) according to Mayring [19] and revolved around the (perceived) presence of halitosis.
The dental examinations were conducted by two calibrated specialized pediatric dentists. Within the first part of the study, the test group (oral preventative program = OPP) received one to four need-based prophylaxis sessions until gingivitis improved (according to PBI, no bleeding) while the control group (treatment as usual = TAU) received one dental prophylaxis session that was adapted to the guidelines of the statutory health insurances with the means of motivational instruction in a professional dental setting. All patients received individualized oral hygiene instructions including the bass technique and a demonstration of interdental cleaning. 3 months after the study onset, all included patients were re-examined and the control group received a single, supplementary, single intensive prophylaxis session (including professional mechanical plaque removal). The final examination of all study patients took place 6 months after the trial had started (Fig. 2). For the secondary analysis focusing on halitosis, the test group (OPP) was regularly instructed to perform mechanical tongue cleaning, which was regularly examined using the Winkel index. The control group (TAU) also received the instruction for mechanical tongue cleaning after 3 months.
Sample size calculationThe present study focused on halitosis as a secondary endpoint; the sample size was calculated for the primary endpoint gingivitis (PBI), using the statistical software package (G* Power, University Düsseldorf). The following a priori parameters were used: expected reduction in gingivitis [20] of 1 PBI value with a standard deviation (SD) 0.7 and non-normally distributed values (non-parametric tests), two-sided analysis, probability of error of 5% and a power of 80%, and a high dropout rate. The calculation resulted in a total of 24 patients, with an additional six assumed drop-outs, which resulted in a two-armed study with 15 patients per group.
Statistical analysesAll statistical analyses were performed using IBM SPSS Statistics 28 (IBM Corp. Released 2021, IBM SPSS Statistics for Windows, Version 28.0. Armonk, NY: IBM Corp). Patient and treatment characteristics were compared by the Mann-Whitney U test for continuous variables and Pearson’s chi-square tests for categorical variables where appropriate. Differences in DMS, HS, MM and Winkel Index between the test and the control group at baseline, 3 and 6 months were analyzed using the Mann-Whitney U test. Wilcoxon rank-sum tests were performed to detect significant changes in DMS, HS, MM and Winkel Index within groups at different time points. Furthermore, correlation analyses were performed to identify correlations between the parameters of interest. Statistical significance was set at p < 0.05.
留言 (0)