CUP is a histologically confirmed metastatic malignant tumor with an unidentified primary site of origin. The clinical presentation of CUP varies among patients [1]. Treatment following the NCCN Ovarian Cancer Guidelines is recommended for patients with adenocarcinoma presenting as intraperitoneal tumors or ascites, where ovarian origin cannot be ruled out based on histological findings [1]. Treatment with either PTX plus CBDCA, docetaxel plus CBDCA, or PTX plus CBDCA plus BV is recommended for epithelial ovarian cancer, fallopian tube cancer, primary peritoneal cancer, and rare histological types [1]
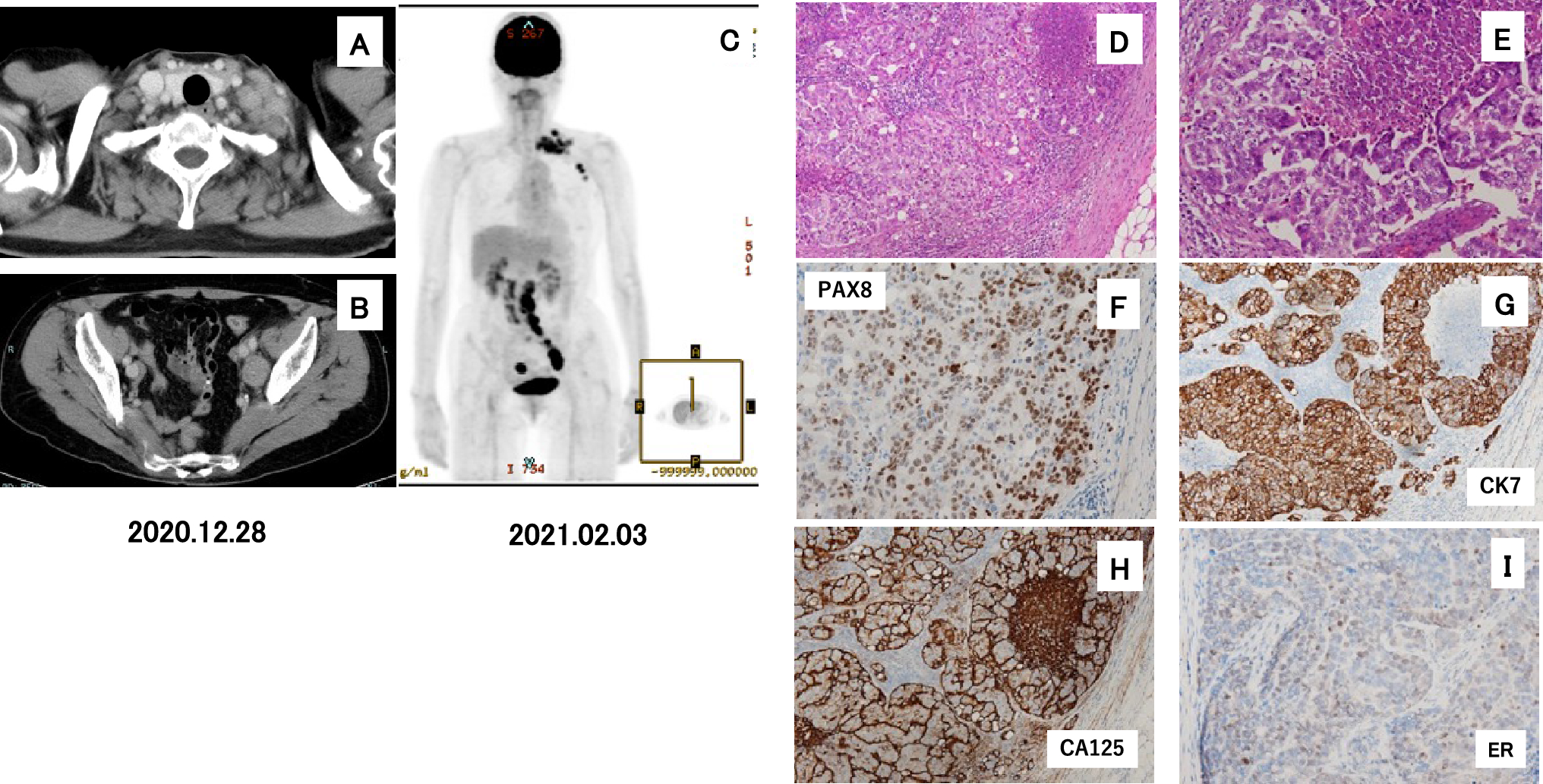
This case demonstrated abdominal lymphadenopathy and elevated CA125, as well as metastases in the left cervical and left axillary lymph nodes, which were slightly exceptional from the typical presentations described in the guidelines.
HBOC syndrome was suspected based on the family history, and BRACAnalysis® was performed, revealing her germline variant in BRCA1 c.L63*. BRCA1,
BRCA1 p.L63* variant is a nonsense variant where codon 63 is changed to a stop codon. Hence, a large BRCA1 protein consisting of 1863 amino acids loses the C-terminal portion distant from codon 63. The BRCA1 c.L63* variant, where all of functional domains are lost, results in the loss of BRCA1-PALB2-BRCA2 trimer formation impairs the homologous recombination function [3]. The BRCA1 p. L63* (NM_007294.4 (BRCA1): c.188 T > A(p.Leu63Ter)) variant is reported as pathogenic in the NIH ClinVar database [5]. A report suggested sensitivity to platinum agents regarding the treatment sensitivity of BRCA1 p.L63* variant [6]. Conversely, no reports have described the clinical sensitivity of PARP inhibitors to this variant, although the sensitivity of this variant to PARP inhibitors using in vitro patient-derived organoids is indicated [6].
An international phase III clinical trial (SOLO-2 trial) revealed that maintenance therapy with the PARP inhibitor Ola demonstrated a significant extension of progression-free survival (PFS) compared to placebo in patients with platinum-sensitive recurrent ovarian cancer with germline BRCA1/2 variants [7]. Investigator-assessed median PFS was significantly longer with Ola (19.1 months, 95% confidence interval [CI]: 16.3–25.7) than with placebo (5.5 months, 95% CI: 5.2–5.8; hazard ratio [HR]: 0.30, 95% CI: 0.22–0.41, p < 0.0001).
Similarly, the ENGOT-OV16/NOVA trial revealed that the PARP inhibitor, niraparib, demonstrated a significant extension of PFS compared to placebo as maintenance therapy in patients with platinum-responsive recurrent ovarian cancer, regardless of BRCA variant status [8]. Patients in the niraparib group had a significantly longer median PFS than in the placebo group, including 21.0 vs. 5.5 months in the gBRCA cohort (HR: 0.27; 95% CI: 0.17–0.41). Our case, for the first time, represents a presumed OCC of CUP with the BRCA1 c.L63* germline variant, which was sensitive to both platinum-based chemotherapy and Ola in clinical practice.
Cases of HBOC syndrome reported as a CUP are extremely rare, and a literature search demonstrated only one reported case from China. A 63-year-old female patient presented with an egg-sized lump in her left iliac fossa with no primary sites. This case demonstrated an embryonic cell variant of BRCA1 (R71K), as well as sensitivity to PTX plus CBDCA, followed by Ola in maintenance therapy, after a tumor resection in the left iliac fossa [9]. This patient survived over 100 months from the onset, and the maintenance treatment with Ola was continued over 16 months in the literature. The patient in our case survives for > 30 months, and the maintenance treatment with Ola was continued for > 25 months.
HBOC syndrome is known to have low penetrance for ovarian cancer unlike familial adenomatous polyposis for colorectal carcinoma. Penetrance estimated by age of 70 years for ovarian cancer was 48.3% and 20.0% for BRCA1 and BRCA2, respectively [10]. However, polyps develop in the early teenage years and result in a nearly 100% lifetime risk of colorectal cancer in cases of familial adenomatous polyposis [11]. Some ovarian cancers in HBOC syndrome may have occult cancer phenotypes. The prevalence of occult ovarian and fallopian tube cancers has been reported at the time of RRSO to be 2.3–23.5% [12]. Low penetrance of ovarian cancer may be responsible for CUP in some cases. Eight (7.8%) occult fallopian tube carcinomas (5 in tubal fimbriae only, 1 in tubal isthmus only, 2 in fimbriae and ovary) were detected in RRSO specimen from 102 women with BRCA genes variants [13]. As ovarian cancer only was 3 (2.9%), existence of the occult fallopian tube carcinomas should be taken care rather than ovarian cancer.
In the future, it is possible that the occult primary lesion would be identified more consistently if RRSO is actively carried out.



留言 (0)