
記住我
What is already known
Heat-producing tools are routinely used during surgical and procedural care. Surgical smoke is a known health hazard to the perioperative team. The evacuation and filtration of surgical smoke reduces workplace injury and improves health outcomes for perioperative staff.What this paper adds
Strategies to address common barriers to surgical smoke management include the development and delivery of annual team education, assessment of the availability of products and equipment, and development and implementation of a risk assessment tool. These strategies for best practices in the perioperative setting are reproducible and can be implemented while taking into account the importance of productivity in this setting. Recommendations for compliance with best practice from lessons learned during this project include establishing early support from frontline staff and the continuation of sustainability strategies, including periodic follow-up audits. INTRODUCTIONWhile performing surgical procedures, surgeons and other health care professionals often use heat-producing tools, such as electrosurgical units, lasers, and powered instruments, to destroy tissue.1 Electrosurgical units and lasers create a smoke by-product, or plume. This by-product may be referred to as surgical smoke, aerosols, cautery smoke, diathermy plumes, plumes, or smoke plumes.2 Surgical smoke is defined as the concentration of ultrafine smoke particles in the air which can contain toxic gases and vapors. These include benzene, hydrogen cyanide, and formaldehyde, in addition to bioaerosols, dead and live cellular material, and viruses.1,3–5 Additionally, current research indicates that several other components are present in surgical smoke, including carbon monoxide, bacteria, nitriles, and polycyclic aromatic hydrocarbons.3 In total, the existing literature has identified up to 377 chemicals in surgical smoke.5 Surgical plume has long been known to contain materials deemed hazardous to the health of health care workers and patients; however, many organizations do not provide protection from exposure to such smoke.2,5 In 1985, the National Institute for Occupational Safety and Health (NIOSH) published a Health Hazard Evaluation Report, stating that there is a “potential hazard from exposure to smoke generated by electrocautery (electrosurgery) knives.”2(p.957)
The debate regarding the harmfulness of surgical plume within the perioperative community remains ongoing. While professional organizations have recognized this potential health hazard for decades, health care organizations have been hesitant to mandate plume-management practices, and there has been little innovation to enhance existing medical devices aimed at reducing surgical plume in the industry.3,4 Proponents of surgical plume evacuation argue that plume presents a significant health hazard to patients and personnel that must be mitigated.3,4 Opponents argue that current evidence-based practice (EBP) recommendations are not conducive to the perioperative setting as they negatively impact efficiency and safety. Dennis reports that it is clear that there is “no such thing as safe smoke.”4(p.103) Surgical smoke exposure has been known to cause a variety of health issues for patients and perioperative staff.4 The chemical components of surgical smoke may be absorbed through the skin and lungs.6 Acute symptoms of smoke exposure may include headache, watering of the eyes, cough, sore throat, nausea, vomiting, weakness, drowsiness, dizziness, sneezing, and rhinitis.6–8 Long-term exposure to surgical plume has been attributed to a higher incidence of lung disease, chronic asthma, emphysema, cancer, and transmission of human papillomavirus. One chemical component, benzene, has been attributed to the development of leukemia.6 Additionally, studies show that over time, surgical smoke can lead to in vitro mutations that contribute to higher rates of pregnancy complications for female surgeons.8
Recommended interventions for surgical smoke evacuation and filtration are consistent among professional organizations and researchers. Current EBP recommendations include mitigation strategies such as risk assessment, smoke evacuation and filtration, consideration of alternative energy-generating devices or surgical techniques, and N95 respirator use.9 Evidence has demonstrated that surgical masks do not provide measurable protection to perioperative staff against surgical smoke.7,9 Surgical mask respirators, such as N95 respirators, may be capable of reducing inhalation exposure to surgical smoke; however, filtering facepiece respirators, such as N100 respirators, are likely the most effective wearable devices for surgical smoke protection.7,9 The Association of periOperative Registered Nurses (AORN) and the European Operating Room Nurses Association (EORNA) recommend using smoke evacuation systems when surgical smoke is present or expected.6,9,10 The EORNA recommendation also includes strong support for the use of personal protective equipment (PPE); however, this recommendation is contradicted by the AORN, which maintains that PPE is the least effective intervention to protect staff.6,10 Current evidence establishes the efficacy of mass-marketed surgical smoke evacuation systems containing high-efficiency particulate air (HEPA) filters.9,11 Additional studies have been conducted validating the efficacy of smoke evacuation accessories, such as electrocautery pencils and in-line suction filters.5 It is also important to consider staff communication strategies and education, as demonstrated by a report on a best practice implementation project conducted in a hospital in Romania.12
While the dangers of surgical plume are widely established, institutional guidance and federal legislation have not been standardized across the US. Approximately 500,000 clinicians of various disciplines are exposed to surgical smoke annually in the US.5 The AORN and the American National Standards Institute have established guidelines and standards of practice that indicate the evacuation and filtration of surgical smoke is necessary to protect patients and health care workers.4 Although the Occupational Safety and Health Administration has acknowledged the hazards related to surgical smoke, the organization has not specifically addressed protection from surgical smoke in its regulatory standards.4 However, as of August 2022, legislation mandating the evacuation of surgical plume has been adopted in nine US states.4
Little evidence exists to gauge compliance with surgical smoke EBPs internationally. The International Federation of Perioperative Nurses, which is composed of member associations representing 40 countries and regions from around the globe, acknowledges the significant risks of surgical smoke in the perioperative setting and recommends standardized smoke evacuation and filtration processes; however, it is unclear if or how these recommendations have been implemented in the international community.13 Denmark is one of the first countries in the world to implement surgical smoke management legislation and remains one of the few to have done so.14 The European Union's directives on the protection of workers from risks related to exposure to biological agents, carcinogens, or mutagens at work establish minimum requirements for member nations to adopt; however, the directives stop short of mandating surgical smoke evacuation.6
The translation of evidence into clinical practice in perioperative settings presents significant challenges across multiple disciplines. This topic was chosen due to a lack of awareness regarding surgical plume management among perioperative staff at the project setting. The project was conducted in the pediatric perioperative setting of a large academic medical center that performs 9,000 surgical procedures annually. The perioperative suite consists of 12 operating rooms located in a new patient-care tower, which opened in November 2020. The center employs approximately 200 frontline staff, including registered nurses, surgical technologists, surgical support staff, certified registered nurse anesthetists, surgeons, anesthesiologists, resident physicians, and students. Each operating room has smoke-evacuator equipment on a ceiling-mounted boom, and one portable smoke-evacuator device is readily available to meet any additional smoke evacuation needs. Although this equipment is available, no formal actions had been undertaken in this setting to evaluate the risk of surgical plume or educate staff on established best-practice standards to protect themselves from the risks associated with surgical plume in the operating room.
The implementation of this best practice project was guided by the JBI Model of Evidence-Based Healthcare15 and used the JBI Practical Application of Clinical Evidence System (PACES) and the Getting Research into Practice (GRiP) audit and feedback strategy16 to implement EBPs for promoting surgical plume management in a pediatric operating room.
OBJECTIVESThe main objective of this project was to promote EBPs regarding surgical plume management in the pediatric perioperative setting of a large academic medical center.
The specific objectives were to:
determine current compliance with EBPs regarding surgical plume management; design and implement strategies to address areas of non-compliance; and perform follow-up audits to assess compliance after implementation strategies. METHODSThis evidence implementation project used the JBI Evidence Implementation Framework.16 This framework is grounded in an audit and feedback process, along with a structured approach to the identification and management of barriers to compliance with recommended practices. It consists of seven stages: (1) identification of practice area for change, (2) engaging change agents, (3) assessment of context and readiness to change, (4) review of practice against evidence-based audit criteria, (5) implementation of changes to practice, (6) re-assessment of practice using a follow-up audit, and (7) consideration of the sustainability of practice changes. These stages are conducted in three phases: (1) implementation planning, (2) baseline assessment and implementation, and (3) impact evaluation and sustainability.
Phase 1: Implementation planningStages 1–2: In Stage 1, the project team identified surgical smoke management as a significant risk to the health and safety of health care workers in the operating room, as the standards of practice outlined by regulatory agencies and professional organizations were not being followed. In Stage 2, stakeholder support was then secured for the project, and included the Chief Nursing and Clinical Services Officer and the Surgeon-in-Chief. The project team included the Director of Nursing, the Nurse Manager (Operating Room), the Nurse Educator (Operating Room), the Clinical Outcomes Coordinator for the department, the Director of Materials Management, and a surgeon champion.
Phase 2: Baseline assessment and implementationStages 3–5: In Stage 3, a context analysis at the project site was conducted by the project team to determine readiness for change and evidence implementation. Eight elements were considered when determining readiness for change: decision-making structure; workplace culture; communication; leadership; resource availability; staff knowledge, skills, and attitudes; commitment to quality management; and interdisciplinary relationships.16 The context analysis revealed significant strengths and challenges within the organization with regard to readiness for change.
In Stage 4, eight audit criteria were developed based on best-practice recommendations for surgical smoke management, as reported in a JBI evidence summary.9 The audit criteria were accessed from the PACES online tool. Table 1 shows the evidence-based audit criteria used in the project (baseline and follow-up audits), together with a description of the sample and method of measuring best practice for each audit criterion.
Table 1 - Audit criteria sample, and method to measure compliance Audit criteria Sample Method used to measure compliance with best practice Audit guide Health care organizations have a policy and procedures for surgical smoke safety. 1 policy review Nurses from the project team confirmed existence of policy and procedures through the PolicyTech database. “Yes” if a policy and procedures are found.The project team determined sample sizes of 25 surgical cases and 30 perioperative staff members for the baseline and follow-up audits. The sample size was approximately 5% of the procedures performed each month and 50% of the total perioperative team, respectively. One policy and procedure review and one product review were also conducted during the baseline audit. The baseline audit was conducted using a random sample from August 15 to September 30, 2022 and entered into PACES.
In Stage 5, the results of the baseline audit were shared through emails and weekly in-person team meetings conducted over a 2-month period (October 1, 2022 to November 28, 2022). Meetings were 1 hour in length and were multidisciplinary, including nursing, physicians, and anesthesiology team members. The results of this audit demonstrated knowledge and practice gaps within the operating room among all disciplines. The use of the GRiP tool aided the project team in identifying barriers to best practice. The team used this information to develop strategies and identify resources to facilitate practice change in the operating room. The authors used the PACES program to guide the GRiP process.
Phase 3: Impact evaluation and sustainabilityStages 6–7: In Stage 6, a follow-up audit was conducted using the same evidence-based criteria and sample sizes as in the baseline audit. The purpose of the follow-up audit was to assess adherence to best practices after implementing strategies targeted to reduce the gap between evidence and practice. Additionally, the follow-up audit results were examined for opportunities to refine the smoke management process and identify any variability in workflow or practice. Process variability was identified between the surgical specialties and teams; thus, the project team implemented additional staff education and reinforced use of the risk assessment tool. This stage lasted from to November 29, 2022 to January 13, 2023.
In Stage 7, the project concluded with consideration given to the sustainability of the new practice changes. The project team determined a schedule for subsequent follow-up audits and assigned a committee responsible for oversight of the project moving forward.
ANALYSISResults data on changes in compliance were measured using descriptive statistics embedded in PACES in the form of percentage changes from baseline.
ETHICSThe project did not require approval from the Institutional Review Board approval. According to the self-certification form and flowchart referenced through the Office of Human Research Protection at the project site, it was not considered research on human participants but a quality improvement project.17
RESULTSDuring Stage 1, the practice area of surgical smoke safety was identified as the issue with the highest potential of causing significant harm to patients and health care workers. During Stage 2, stakeholders were identified and their engagement was secured. A project team was established and responsibilities were identified. The Director of Nursing maintained oversight of the project implementation and worked closely with the Nurse Manager, Nurse Educator, Clinical Outcomes Coordinator, and Director of Materials Management to identify and implement strategies to overcome barriers to best practice. The Nurse Manager was responsible for the oversight of day-to-day operations and staff compliance. The Nurse Educator's responsibilities included staff education and data collection. The Clinical Outcomes Coordinator was responsible for data collection and reporting. The surgeon champion provided technical knowledge and support through the product evaluation and implementation processes. During the context analysis in Stage 3, the project team identified positive indicators of readiness for change in the decision-making structure, workplace culture, leadership, commitment to quality management, and interdisciplinary relationships. Challenges were identified related to communication; resource availability; and staff knowledge, skills, and attitudes.
In Stage 4, 25 surgical procedures and 30 perioperative staff members were randomly selected for the baseline audits for Criteria 5 to 7. Criteria 1 to 4 were each assessed once during the baseline audit period via one policy and procedure review and one product review to determine compliance, indicating a sample size of one. The surgical procedures consisted of elective, scheduled cases for which heat-generating surgical tools were available. The perioperative staff were randomly selected from the staff roster and consisted of registered nurses and surgical technologists.
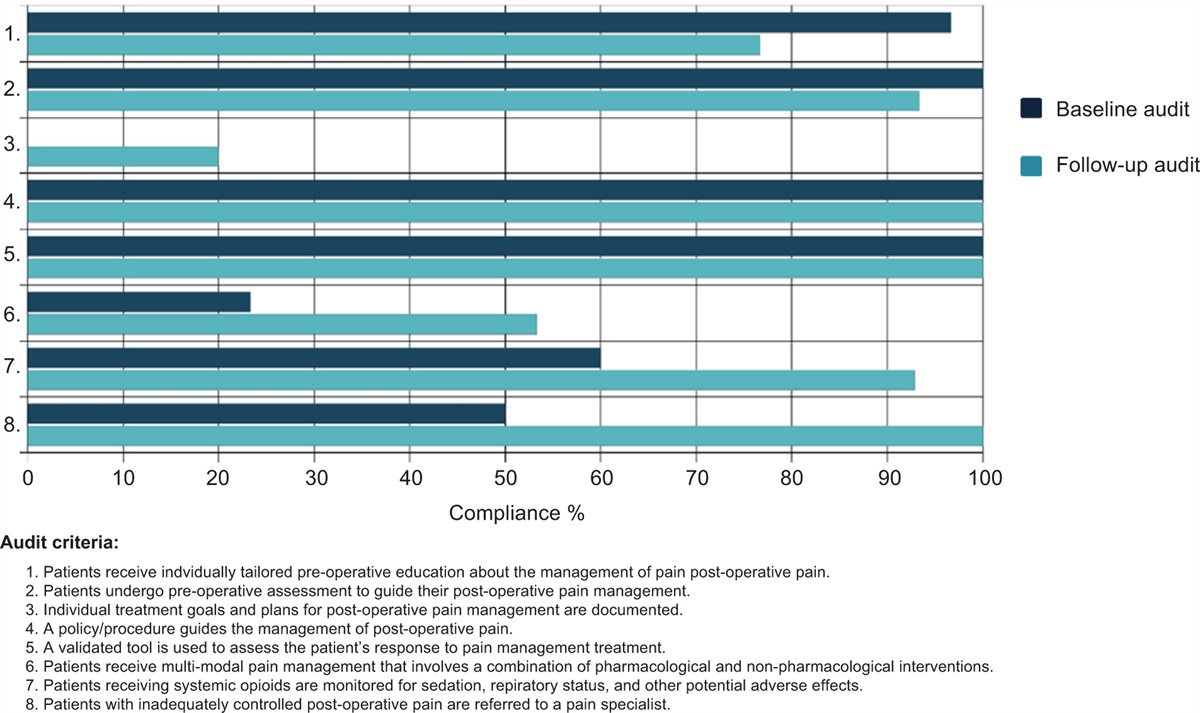
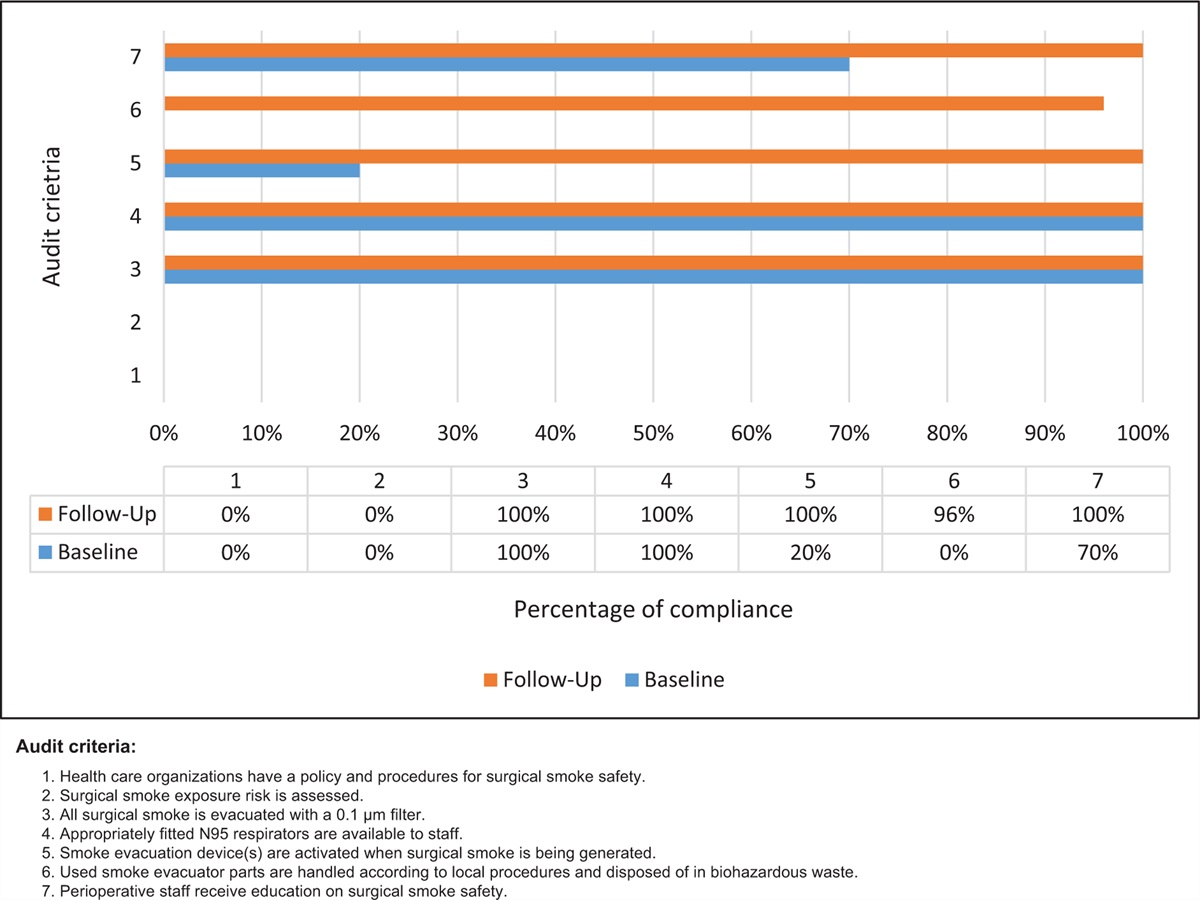
The criteria with the highest compliance (100%) were Criterion 3 (n = 1): All surgical smoke is evacuated with a 0.1 μm filter, and Criterion 4 (n = 1): Appropriately fitted N95 respirators are available to staff. The second highest percentage of compliance (at 70%) was Criterion 7 (n = 30): Perioperative staff receive education on surgical smoke safety. This criterion was dependent upon the department having performed and documented surgical smoke safety education for employees upon hire. Compliance with Criterion 5 (n = 25): Smoke evacuation devices are activated when surgical smoke is being generated was found to be at 20% compliance. Criterion 1 (n = 1): Health care organizations have a policy and procedures for surgical smoke safety, Criterion 2 (n = 1): Surgical smoke exposure risk is assessed, and Criterion 6 (n = 25): Used smoke evacuator parts are handled according to local procedures and disposed of in biohazardous waste were the poorest performing measures at 0% compliance.
In Stage 5, a GRiP analysis (Table 2) was used to review the findings of the baseline audit, identify barriers and enablers to the utilization of EBPs, and develop implementation strategies to improve compliance. Three barriers were identified. The first barrier was the lack of staff knowledge about surgical smoke management best practices, which was critical for Criteria 2, 3, 5, 6, and 7. The baseline audit showed that 70% of surveyed staff had some mention of surgical smoke management education in their educational records; however, it was determined that the content of the education was variable and did not reflect current EBP recommendations. The project team developed and delivered an educational module (see Appendix I, https://links.lww.com/IJEBH/A154). on surgical smoke management to perioperative staff via in-service education and the institution's electronic learning management system. This module was integrated into the annual mandatory continuing education schedule and the new hire onboarding program.
Table 2 - Getting Research into Practice (GRiP) analysis Barrier Strategy Resources Outcomes • Lack of staff knowledge about surgical smoke management best practices. • Develop and deliver annual education on evidence-based practices.The second barrier identified was that there was no existing process for assessing surgical smoke exposure risk as defined in Criterion 2. The strategies to overcome this barrier were to develop and implement a surgical smoke exposure risk assessment tool and develop and deliver education on surgical smoke exposure risk assessment to perioperative staff. The project team developed a surgical smoke exposure risk assessment tool which was printed, laminated, and posted in the operating rooms for reference for the perioperative staff (Appendix II, https://links.lww.com/IJEBH/A155). The tool allowed staff to determine whether surgical smoke exposure risk was present using pre-determined questions regarding the procedure. Staff education on the new tool was integrated into the educational module developed for the first barrier.
The final barrier was the limited availability of smoke evacuation disposables, which directly correlated with Criteria 3 and 6. The project team conducted a thorough, multi-disciplinary product assessment of readily available products, including smoke evacuator equipment, pencils, and suction devices. Using this data, the team conducted a gap analysis and determined that perioperative staff had no access to in-line HEPA filters and that there were no established periodic automatic replenishment (PAR) levels for existing devices and consumables. As the hospital had not mandated surgical smoke evacuation in its operating rooms, materials management had not sourced or routinely stocked the equipment and supplies necessary to follow evidence-based recommendations. The project team sourced and evaluated a new in-line HEPA filter and established PAR levels on the new and existing supplies and equipment.
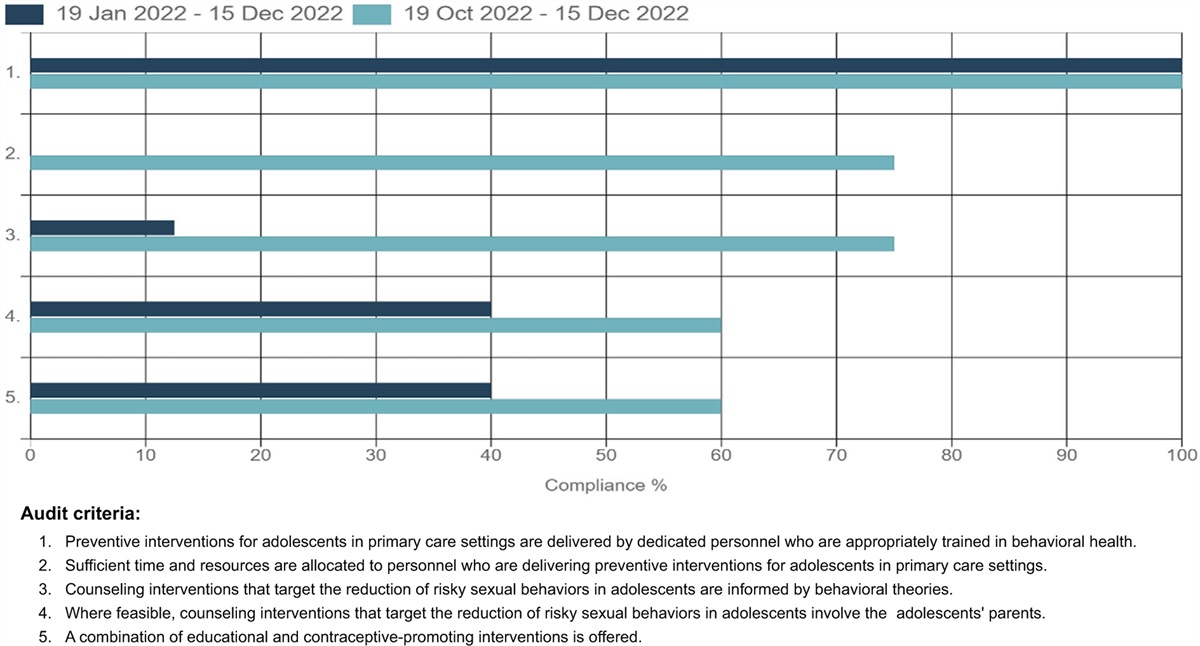
In Stage 6, a follow-up audit was conducted after strategies had been implemented. Figure 1 shows the results of the baseline and follow-up audits. The comparison shows an overall improvement in compliance with Criteria 5, 6 and 7, with 80%, 96%, and 30% improvement noted, respectively. No changes were noted for Criteria 3 and 4, which were at 100% at baseline. No improvement in compliance was noted for Criteria 1 and 2, as no policy and procedures for surgical smoke safety had been adopted by the institution during the project period.
 Figure 1:
Figure 1: Compliance (%) with best practice for audit criteria for surgical smoke at baseline and follow-up.
In Stage 7, the project team decided that quarterly audits should be conducted to monitor progress with EBP compliance and to continue to identify opportunities for improvement. Quarterly audits will be performed by nurse and physician leaders within the department and reported to the department's Quality and Safety Committee for ongoing review and management. Oversight of the ongoing educational module will be maintained by the department's nurse educator and updated as new guidelines and EBPs become available. This work will continue past the end date of the project as the risk assessment tool will be built into the electronic medical records to support documentation and future compliance audits.
DISCUSSIONThe objectives of this implementation project were to determine baseline compliance with EBPs regarding surgical plume management, design and implement strategies to address areas of non-compliance, and perform follow-up audits to assess compliance after improvement strategies were implemented. The project was conducted in the pediatric perioperative setting of a large academic medical center. Twenty-five surgical cases and 30 perioperative staff files were reviewed for the baseline audit. Additionally, one policy and one product review were conducted. Data from the baseline audit allowed the project team to identify barriers to compliance with best practices. The team used the GRiP process to identify and apply strategies to address these barriers. After the strategies were implemented, a follow-up audit was conducted using the same sample size as in the baseline audit. Comparison between the two audit sets provided insights for further recommendations.
The follow-up audit showed an increase in compliance for Criterion 5, where smoke evacuation devices are activated when surgical smoke is being generated. It was determined by the project team that compliance likely increased due to the enhanced availability of appropriate smoke evacuation equipment. To increase the availability of equipment, leaders engaged frontline staff and surgeons to elicit support. Both groups were slow to offer support to the initiative; however, once education was provided on the hazards presented by surgical smoke in the operating room, many staff and surgeons became proponents of the evidence-based changes. The project team found that while the surgeons were the primary end-users of smoke-generating devices, the operating room staff, including the circulating nurses, surgical technologists, and anesthesia personnel, had immense influence on surgeon practice and choice of equipment. Therefore, while all perioperative staff were important to the success of the project, the frontline staff were the true key stakeholders promoting change. There was also an increase in Criterion 6, where used smoke evacuator parts are handled according to local procedures and disposed of in biohazardous waste. While compliance with both Criteria 5 and 6 increased significantly, there was not a direct correlation between barriers, as had been expected by the project team. Criterion 6 had never been discussed at the departmental or institutional level within the organization and resources were not immediately available to address the associated educational barrier. Additionally, there was an increase in compliance for Criterion 7, where perioperative staff receive education on surgical smoke safety. The project team believed that an increase in compliance with this criterion would have positively affected Criteria 5 and 6.
No changes were noted for Criteria 3 and 4, which were already at 100% at baseline. The project site had previously attempted to implement widespread smoke evacuation resources in the perioperative areas and thus, the appropriate filters and N95 respirators were already available to staff during the audit periods. Due to the exacerbation of supply chain-related challenges caused by the COVID-19 pandemic, smoke evacuation supplies were difficult to obtain after they had been sourced and ordered. Further recommendations are needed to identify alternative smoke evacuation devices, equipment, and supplies in the event of a widespread supply chain-related event.
No improvement in compliance was noted for Criteria 1 and 2, as no policy or procedures for surgical smoke safety were adopted by the institution during the project period. The project site is part of a large, multi-campus academic medical center with multiple perioperative areas that share policies and procedures. The project team determined that limiting the project's scope to the pediatric perioperative department was necessary for the project to move forward. The project team developed a surgical smoke exposure risk assessment tool and a policy proposal as part of the project. The surgical smoke exposure risk assessment tool was developed and implemented as a visual aid at the project site to assist staff with evidence-based decision-making; however, due to the limited scope of the project and pre-existing EMR limitations, the tool was not added to the EMR to allow staff to document the surgical smoke safety interventions. It was determined by the EMR team that the addition of the tool could not be site-specific and thus, it would also affect the non-participating departments. Similarly, an institutional policy would also affect the non-participating departments, so it was determined that the project team would develop and submit the policy proposal to the institution's perioperative leadership team for review. The project team recommends the future adoption of both documents by the organization and the implementation of the risk assessment tool in the institution's EMR.
The project team determined that the most critical strategy to maintain future compliance, affecting Criteria 5 to 7, would be continuing education on smoke evacuation EBPs. Employee safety initiatives in health care have become more widespread over the last several years; however, staff in the operating room are less likely to consider surgical smoke exposure to be a hazard compared with needlesticks and musculoskeletal injuries, which receive much more attention at the institutional level. Surgical smoke exposure is a known hazard that affects only a small percentage of health care workers and thus, little attention is paid to the issue by many large health care organizations. As such, the project team determined that prior educational efforts by the organization were almost non-existent. Due to leadership turnover in the department, little oversight exists with regard to the continuing education requirements for nursing staff and physicians in the operating room. Additionally, physicians in the organization do not receive mandatory continuing education outside of the requirements of their academic department. Oversight of the ongoing educational module developed during this project will be maintained by the department's Nurse Educator and updated as new guidelines and EBPs become available. The project team recommends that surgical smoke safety education also be mandated for all perioperative physicians, including resident and attending physicians, and other advanced providers working in the department. This education should be completed upon initial hire and renewed annually.
To ensure consistency and future compliance with EBPs, the project team will turn over control of the initiative to the department's Quality and Safety Committee for ongoing review and management. Follow-up audits will be performed by nurse and physician leaders within the department and reported to the committee quarterly.
Limitations of the project included supply chain and staffing challenges, in addition to the overall scope of the project and timeline. Due to the limited scope, two audit criteria were largely unaffected by the project's strategies. Additionally, the time gap between the baseline and follow-up audits was limited to 2 months and represents a limitation, both for the implementation and sustainability of the project.
CONCLUSIONSSurgical smoke is potentially harmful to the health and well-being of perioperative staff.5 As exemplified during the COVID-19 pandemic, the safety of health care workers is of paramount importance in the delivery of patient care. This project aimed to promote evidence-based surgical plume management in the pediatric perioperative setting of a large academic medical center. The project succeeded by improving average compliance by 30% in five of the seven audit criteria. Perioperative leaders will need to monitor education to promote continued compliance. Further work is needed within the organization to fully implement strategies to address Criteria 1 and 2. The adoption of an institutional policy and procedures is required to ensure the consistent application of EBPs across the organization. The surgical smoke risk assessment tool developed by the project team should be built into the EMR and a workflow identified and implemented to ensure appropriate use and documentation of interventions.
Although the purpose of this project has been achieved, further audits are needed to ensure continued compliance. It would be advantageous to explore any correlation between increased compliance with EBP criteria and the health status of perioperative staff. While some case studies and case series have been conducted on the short-term impact of surgical smoke exposure among members of the perioperative team, no large-scale cohort studies have been completed to examine the potential long-term impacts. The ability to demonstrate the importance of EBPs to staff opposing practice change will continue to improve compliance and foster a culture of safety for all involved in care delivery.
ACKNOWLEDGMENTSThe authors would like to thank Children's of Mississippi and the University of Mississippi Medical Center School of Nursing for providing the opportunity and support for this project.
DECLARATIONSHM is a perioperative registered nurse. This report will contribute toward a Doctor of Nursing practice degree for HM.
留言 (0)