
記住我

The present study retrieved CBCT examinations from a 2016/2017 study [14] that had received ethical approval by the Swedish Ethical Review Authority (Daybook no. [Dnr] 2016/422-31, 2019-04106) [20]. Thus, participants received no ionizing radiation in the present study. The Swedish Ethical Review Authority approved the present study (Dnr 2023-01170-01) [20], which was conducted according to the principles of the Declaration of Helsinki, and the guidelines of the International Commission on Radiological Protection (ICRP) in Biomedical Research [21]. Karolinska Institutet in Stockholm, Sweden, anonymized all CBCT images before sending them to our research group at the Faculty of Odontology in Malmö, Sweden. The only information we received was the sex and age (in years) of the patients at the time of the examination.
Study design and participantsCBCT examinations of 68 pediatric patients (age range 7–15 years) with non-syndromic clefts involving the alveolar process were carried out in 2016–2017 at Karolinska Institutet in Stockholm, Sweden. One CBCT examination was made for each patient, either before or after alveolar bone grafting. The purpose was to evaluate the anatomy of the anterior maxilla, before or after alveolar bone graft surgery [14]. Fifty-three CBCT examinations were exposed prior to bone graft surgery and 15, after bone graft surgery using a Promax 3D Mid scanner (Planmeca Oy, Helsinki, Finland). Thirty-five volumes were exposed with a standard-dose protocol and 33, with an ultra-low-dose protocol. Both were protocols defined by the manufacturer. The standard-dose protocol had a tube current of either 6 or 8 mA, depending on the size of the patient, and an exposure time of 12 s. The ultra-low-dose protocol had a tube current of either 4 or 5 mA, depending on the size of the patient, and an exposure time of 4 s. Both protocols had a tube voltage of 90 kV. All CBCT images had the same voxel size of 0.2 mm3 and a field of view of 8.0 × 5.0 cm. The dose area products were 482 and 612 mGy cm2, respectively, for the tube currents of 6 and 8 mA in the standard-dose protocol, and 114 and 141 mGy cm2, respectively, for the tube currents of 4 and 5 mA in the ultra-low-dose protocol.
CBCT examination reviewOne junior oral and maxillofacial radiologist (AV) with 5 years of experience in oral radiology evaluated all CBCT examinations (n = 68) under dimmed-light conditions. Reviews of the first ten cases were done under the supervision of two senior oral and maxillofacial radiologists (X-QS, KHH), each with more than 10 years of experience in oral radiology. In cases of doubt or disagreement, consensus was reached within the group (AV, X-QS, and KH-H). The technical settings of all CBCT examinations were extracted with ImageJ software (ImageJ, version 1.53q, US National Institutes of Health, Bethesda, Maryland, USA). Tube voltage, exposure time, tube current, dose area product, and field of view as well as voxel size were noted.
Table 1 summarizes the parameters evaluated in the CBCT examinations and Figs. 1, 2 and 3 present examples. All parameters, apart from cleft volume, were evaluated using Planmeca Romexis software (Romexis, version 6.0, Helsinki, Finland).
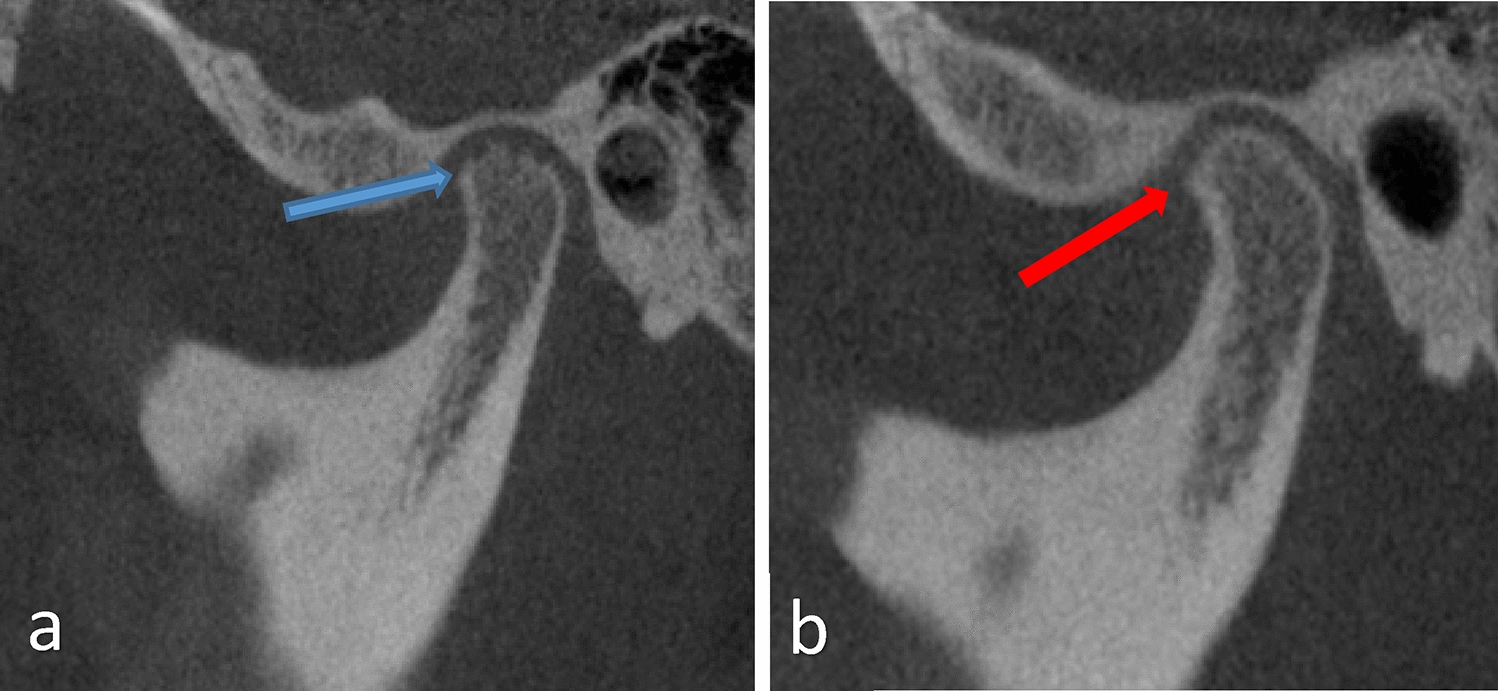
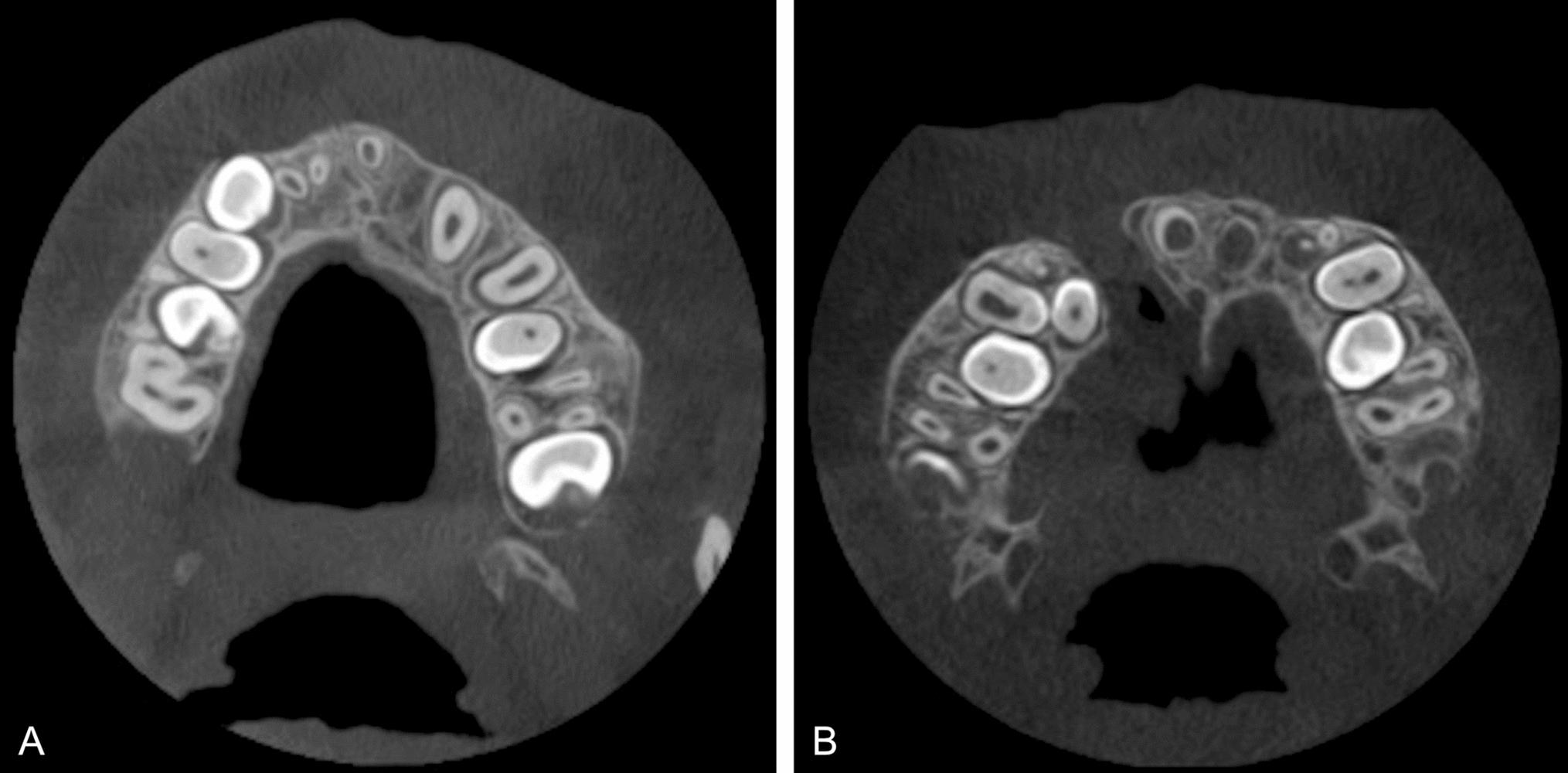
Table 1 Parameters collected from cone beam computed tomography (CBCT) examinations of 68 pediatric patients with cleft lip and/or palateFig. 1
Visibility of the incisive foramen: A completely visible, B partially visible
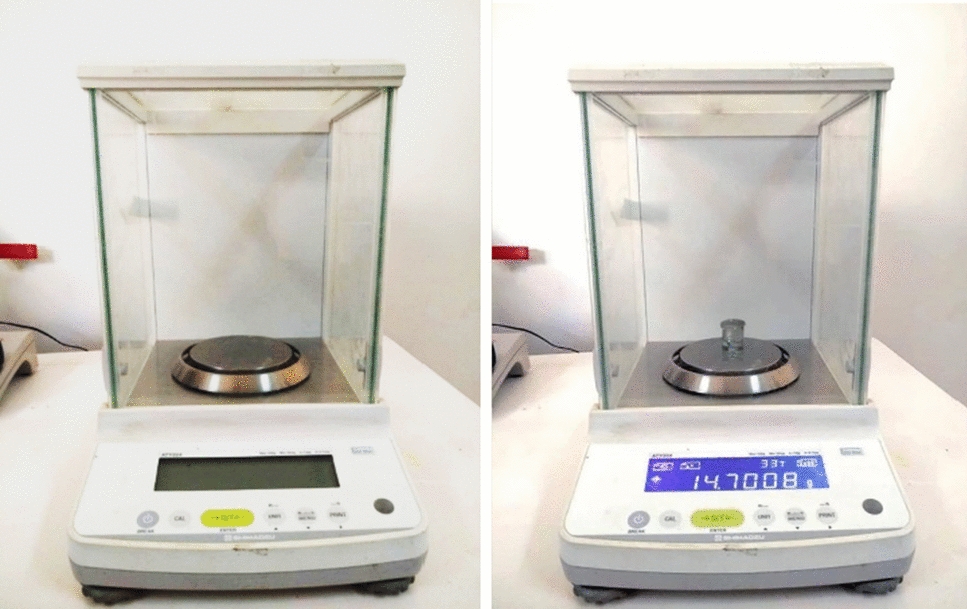
Fig. 2
Example of determining the size of the widest part of the inferior turbinate
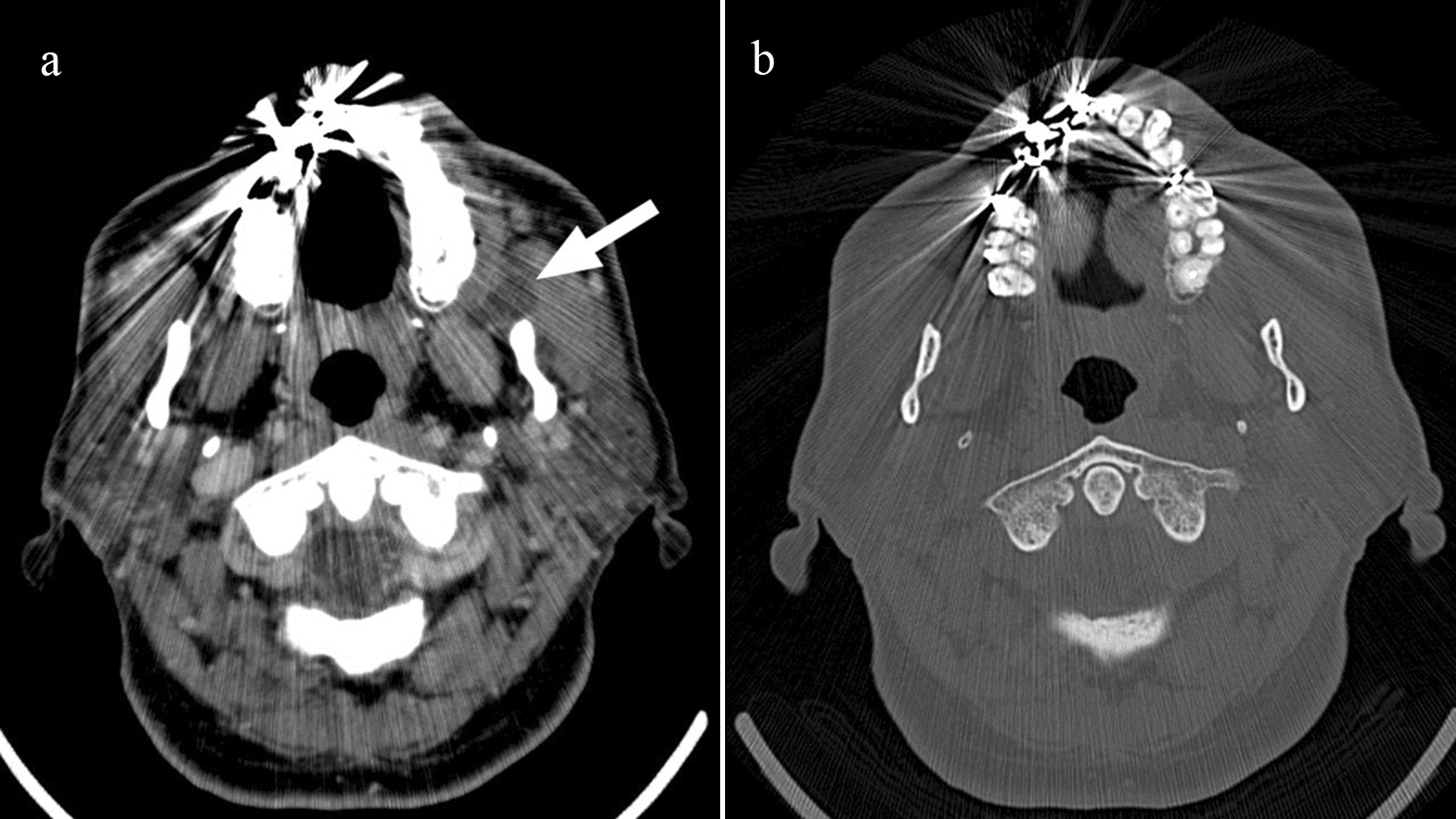
Fig. 3
Comparison of the location of the nasal floor between the graft side (right side) and the non-cleft side (left side)
Volume determinationCleft volume in the 53 pre-operative CBCT examinations was determined using Bruker CTAn Micro-CT software (Bruker CTAn Micro-CT, version 1.15.4, Billerica, MA, USA). The examinations were imported in DICOM format.
The anatomical reference point for the superior border of the cleft was defined as the nasal floor of the non-cleft side in cases with unilateral clefts and as the expected nasal floor in cases with bilateral clefts. The inferior border was defined as the marginal part of the alveolar crest, where the enamel cement junction of adjacent teeth was visible. The buccal, palatal, mesial, and distal borders of the cleft were roughly defined manually on all axial cross-sectional images (Fig. 4).
Fig. 4
Definition of the cleft area (in red)
The software calculated the volume of the cleft, taking account of the limits imposed by the user. These included the volume within the borders of the cleft as described anteriorly and excluded structures and tissues that should not be considered part of the cleft, such as tooth substance. Volume was calculated in cubic pixels and then converted into cubic centimeters.
Statistical analysisAll data were registered and analyzed in the Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows, version 27.0. Armonk, NY: IBM Corp). Frequency analyses were performed, and cross-tabulations were analyzed. The statistical tests used included the t test for comparison of cleft volumes and the mean size of the inferior turbinates, and the ordinal regression analysis for evaluating the visibility of the incisive foramen. The significance level was set at p ≤ 0.05.
留言 (0)