This study is, to our knowledge, the largest to compare the laparoscopic and robotic Pancreatoduodenectomy, and the first to do so using propensity-matching to reduce confounding variable bias. We find that, when matched for potential confounders, the two approaches have similar rates of readmission, mortality, length-of-stay and completion of neoadjuvant therapy. We also find that the two approaches can achieve similar short-term oncologic success as measured by the nodal harvest and the rate of positive margins. We do conclude, like previous studies, that outcomes are best when performed in higher-volume centers, with improvement at a center-volume of at least 5 cases per year. [12, 13].
There has been a significant amount of data comparing open and minimally invasive pancreatectomy, with the general consensus that MIPD is, at least, a safe approach. Croome et al. showed that LPD was associated with a reduced LOS and an improved rate of initiation of adjuvant therapy versus OPD [14]. Stauffer et al. subsequently showed a similar survival rate, but with a greater nodal harvest in LPD vs OPD [15]. Subsequent analysis in large cohorts shows generally improved short-term outcomes with LPD, including reduced LOS at the cost of longer operative time; there is no reported difference in long-term oncologic outcomes between open and laparoscopic PD [16,17,18,19]. However, as case volumes in robotic surgery continue to rise, differences between laparoscopic and robotic approaches may influence the perceived outcomes of MIPD [20,21,22]. Previous smaller studies, such as Nassour et al. (2017), have found no difference in postoperative complication rates, but a reduced conversion rate with RPD [23,24,25]. The presented study represents this most modern cohort for this analysis and is the first propensity-matched analysis on the topic. Incorporating both perioperative and short-term oncologic outcomes, including initiation of adjuvant chemotherapy, which is often cited as a success metric in oncologic surgery, this study suggests that both RPD and LPD are technically appropriate and feasible approaches to this complex procedure based on provider comfort. This is particularly helpful in the setting of the recent LEOPARD trial demonstrating improved outcomes of the MIPD versus the open approach [26].
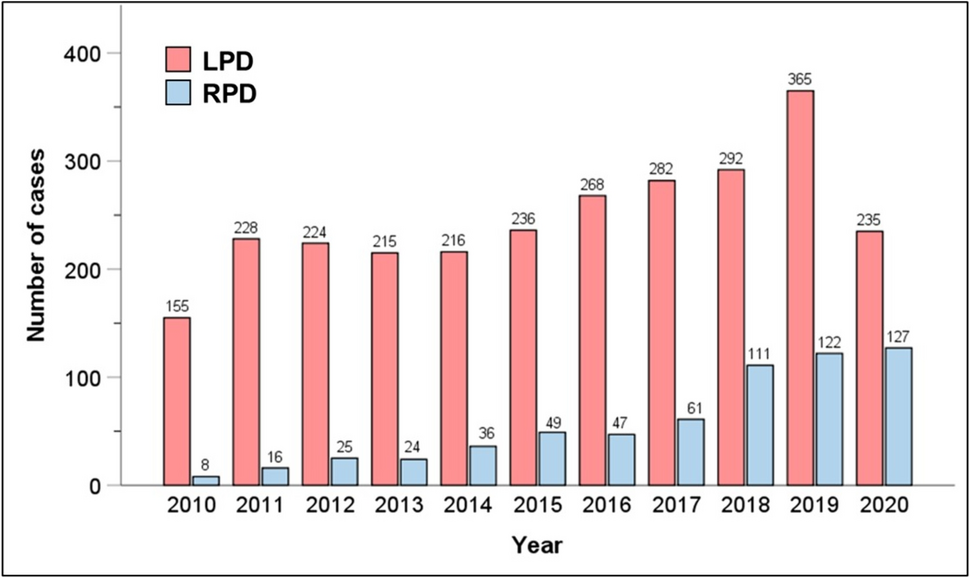
The concept of a “learning curve” in surgery, particularly with respect to minimally invasive surgery, has now been well established in impacting surgical outcomes [12, 27,28,29]. This is particularly true in pancreatic surgery, where outcomes are highly correlated with both personal and center-level case volumes [30,31,32]. However, given the more recent rise of MIPD, this concept is somewhat less studied in this cohort. Conroy et al. [33] and Adam et al. [34] both used larger databases to establish cut-offs of annual case-volumes associated with reduced complications, identifying 20 and 22 cases/year, respectively, as the target for improving outcomes [33, 34]. The former of these studies did utilize an older version of the NCDB for their analysis, while the Adam et al. article employed the National Inpatient Sample (NIS) up to 2012 [33]. Annual case volumes of RPD have nearly doubled from 2017 to 2020 compared with those prior to 2017, with RPD representing over 50% of MIPD cases in recent years (Fig. 1). Thus, by including more recent years, and confirming adequate representation of both RPD and LPD, we provide a modern, holistic assessment of the impact of learning curve on the outcomes of MIPD, confirming the findings of prior studies that higher case volumes do improve outcomes. While it is interesting that not all outcome metrics are volume-dependent, there is a clear trend toward improved technical and post-operative outcomes in high-volume centers. This could be considered a modifiable risk factor, wherein dedicated surgeons or surgical groups can place effort to improve patient care. We also found that improvement in outcomes happened upwards of 5 cases/year for the MIPD, which represented the upper two quartiles in analysis, and may represent an annual volume needed to progress along the learning curve. This is somewhat lower than the previously cited studies and shows that the target number is not so high as to unachievable by many centers nationwide [33, 34]. It is also notable that increasing use of the robotic platform does not eliminate the importance of experience. Thus, while robotic surgery is useful and exciting, it cannot replace diligent training or thoughtful repetition. We do want to note that this is a conceptual finding regarding surgeon experience, and there should not be a specific cut-off below which centers are considered “low volume”.
This study has limitations. Most notably are the inherent detriments of using large databases. While this allows us to increase sample size and generalizability, it also precludes detailed analyses of why a certain approach was chosen and may introduce confounding biases. We attempted to control for this by propensity-matching, but this cannot completely remove the potential for between-group bias. The NCDB does not record overall complication rates. Thus, mortality, readmission and initiation of adjuvant chemotherapy were employed as surrogate markers, but we cannot truly assess overall complication rates. Further, the NCDB, unlike NSQIP, does not include a granular report on postoperative morbidities like DGE, POPF, and many others that are pertinent to pancreatoduodenectomy. However, NCDB allows the aggregation of surgical cases by institutional codes to gauge annual volumes. NSQIP de-identifies this data which prohibits performing outcomes research based on institutional volumes. Moreover, NSQIP does not provide data on adjuvant therapies, and only recently started providing oncologic quality metrics like nodal harvest. After careful evaluation of both databases, we chose to go with NCDB which better serves the purpose of our clinical question, yet this then mandates that we employ length-of-stay, readmission rates, and mortality as general surrogates for the postoperative course. However, as mentioned, granular data regarding complication rates is not available, which is a limitation of this study. Finally, this study was not able to assess long-term oncologic outcomes, which may vary between groups. Short term-surrogates, including margin-positive resection, nodal harvest and initiation of adjuvant therapy were used in an attempt to address oncologic outcomes but this cannot be confirmed to translate into long-term equivalency.


留言 (0)