
記住我

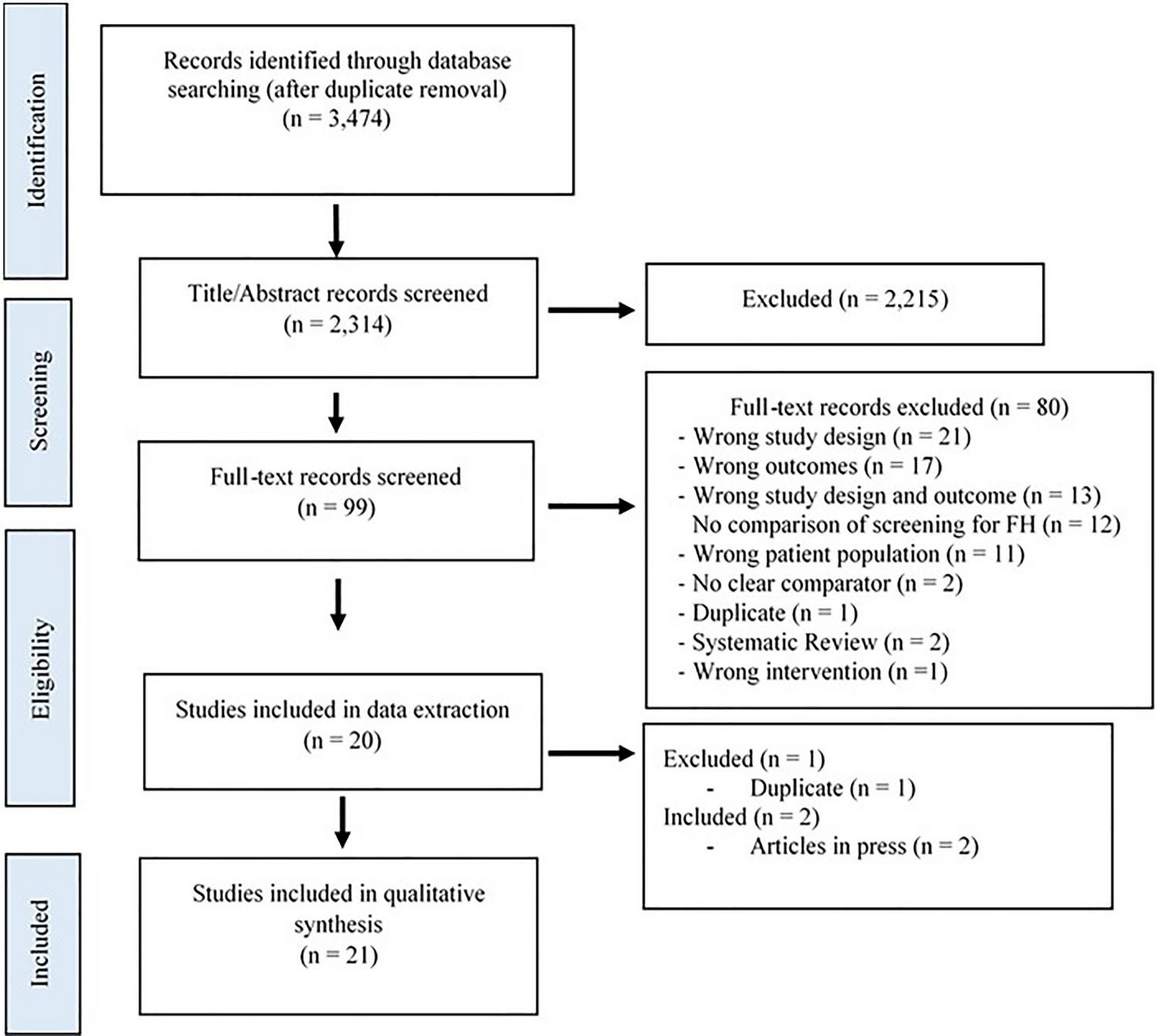
A decision-analytic model with a Markov structure and a 1-month cycle length was developed in Microsoft Excel to assess initiating PrEP with CAB–LA versus generic daily oral FTC/TDF (Fig. 1). The model used a lifetime time horizon to fully capture all costs and effects, as HIV-1 infection requires lifelong management. The modeled population included MSM, TGW, and cisgender women aged 18 years and older who are at an increased risk of acquiring HIV-1 infection. At the initiation of the model, individuals were assumed to experience this increased level of risk for a total of 5 years. This duration of increased risk was estimated by calibrating modeled lifetime risk of HIV acquisition without PrEP against US lifetime HIV-acquisition estimates [16]. Longer and shorter durations of risk were tested in the scenario analysis.
Fig. 1
Model Overview Diagram. CAB–LA cabotegravir long-acting, FTC emtricitabine, MSM men who have sex with men, PrEP pre-exposure prophylaxis, TAF tenofovir alafenamide, TDF tenofovir disoproxil fumarate, TGW transgender women. aFTC/TAF is not approved for use in cisgender women
Individuals entered the model by initiating CAB–LA or generic daily oral FTC/TDF. Over time, individuals could continue receiving their initial PrEP option, transition to a second PrEP option, or discontinue PrEP. In the CAB–LA pathway, the second PrEP option for all individuals was generic daily oral FTC/TDF. In the oral PrEP pathway, the second PrEP option for MSM and TGW was daily oral FTC/TAF; cisgender women in the oral PrEP pathway did not have a second PrEP option because FTC/TAF is not approved for individuals at risk of HIV acquisition from receptive vaginal sex. While receiving PrEP, individuals were at a lower risk of acquiring HIV-1 infection than those not receiving PrEP, with protection levels dependent on their selected PrEP option and their PrEP adherence and persistence. Individuals receiving PrEP also completed ongoing monitoring visits and testing in accordance with CDC guidelines [6, 17,18,19], and those receiving CAB–LA could experience injection site reactions (ISRs) [9, 10, 20].
Individuals who acquired HIV-1 infection discontinued use of PrEP and transitioned to HIV-related care, including multiclass antiretroviral (ARV) treatment regimens, ongoing monitoring, and other related care, for the remainder of their lifetimes. Individuals with unsuppressed HIV-1 infection could also transmit HIV onwards or develop PrEP-related resistance mutations. Individuals who did not acquire HIV-1 infection during the 5-year duration of risk were assumed to incur no additional costs for the remainder of their lifetimes.
The analysis took a healthcare sector perspective and assessed costs and health outcomes for the eligible cohort over time. Input parameter values were obtained via a targeted review of public and published sources. The most recent relevant source was selected when multiple sources for an input were available. Modeled cost outcomes in 2022 US dollars included PrEP-related costs (e.g., drug acquisition, administration, monitoring, and adverse event management costs) and lifetime costs associated with new HIV-1 infections. Health outcomes included new primary and secondary HIV-1 infections and the associated losses in life expectancy and quality-adjusted life-years (QALYs). Average per-person costs and health outcomes were discounted at 3% per year, according to established US cost-effectiveness practice recommendations [21], and various incremental cost-effectiveness ratios (ICERs), such as the incremental cost per QALY gained, were then calculated to compare PrEP scenarios.
2.2 Modeled PopulationThe population entering the model included adults with increased risk of acquiring HIV-1 infection and eligible to receive PrEP [1]. The base-case analysis focused on PrEP-eligible populations aligned with the HPTN 083 and HPTN 084 study populations. The modeled distribution of MSM and TGW (HPTN 083) and cisgender women (HPTN 084) is presented in Table 1. In the scenario analysis, the cost-effectiveness of CAB–LA was assessed for specific population subgroups, including MSM and TGW, African American/Black MSM, Hispanic MSM, White MSM, and cisgender women.
Table 1 Model inputs: population characteristics and HIV health effects2.3 PrEP UseThe model accounted for PrEP adherence, persistence, and switching, with parameter values specific to each PrEP option. All PrEP-use parameters and assumptions for the base-case analysis are provided in Table 1.
2.3.1 PrEP AdherenceAdherence is a critical factor in PrEP efficacy, and many individuals receiving oral PrEP have documented adherence issues due to known barriers such as daily pill burden, stigma, and concerns about potential side effects [22, 23]. Nevertheless, oral PrEP requires a high level of adherence to be effective (ideally 4+ doses per week for MSM and TGW [6] and 6+ doses per week for cisgender women [4, 5]). CAB–LA injections are directly administered by a healthcare provider and may address adherence barriers associated with oral PrEP [22, 23]. In the HPTN 083 clinical trial, 70.0% of a random sample of participants in the FTC/TDF arm had laboratory evidence via dried blood spot testing consistent with four or more doses per week [24]. In contrast, 91.5% of person-years (PY) were covered in either arm of the trial by CAB–LA or placebo injections, defined as injections received with a delay of less than 2 weeks [9] [note that the dosing schedule approved by the Food and Drug Administration (FDA) states that CAB–LA may be given up to 7 days before or after the date the individual is scheduled to receive their injection [11].] To account for the observed adherence, the base-case analysis adjusted acquisition costs downward for oral PrEP (assuming less frequent prescription refills; see Online Resource for more information) and, conservatively, used full, unadjusted costs for CAB–LA based on indicated dosing. For both CAB–LA and oral PrEP, efficacy did not require adjustment in the base-case analysis, as it was already aligned with observed clinical trial adherence. In the sensitivity and scenario analyses, adherence to oral PrEP was varied using uncertainty information and real-world adherence data [7]; these changes were allowed to affect PrEP costs and efficacy (see Online Resource for more information). A similar analysis has not yet been conducted for CAB–LA due to a lack of data on the impact of changes in CAB–LA adherence on efficacy.
2.3.2 PrEP Persistence and SwitchingPersistence on PrEP was defined as the percentage of modeled individuals remaining on PrEP over time. Oral PrEP persistence was taken from a study assessing real-world PrEP persistence in the USA over a 12-month period [7]. As expected, a higher rate of PrEP discontinuation was observed during the initial 6 months of use than in months 6–12. Accordingly, the model assumed a higher rate of PrEP discontinuation in the first 6 months followed by a lower rate from that point onward, with a consistent value based on discontinuation observed between 6 months and 12 months in the real-world study [7]. CAB–LA persistence in the real world had not yet been assessed at the time this model was developed. As CAB–LA provides an additional modality that addresses barriers to both adherence and persistence [22, 23], it may improve PrEP continuation rates. This trend would be consistent with the experience in contraception, where matching women’s preferred modality increased persistence [25]. Therefore, CAB–LA was assumed to have a 20% relative improvement in persistence compared with oral PrEP at all time points. Equal persistence was tested in the scenario analysis. In all cases, individuals who discontinued their initial PrEP could switch to another option (Table 1). Conservatively, the model did not account for any residual CAB–LA efficacy after discontinuation. This assumption is consistent with guidelines that recommend initiation of daily oral PrEP within 8 weeks after the last injection of CAB–LA for individuals at continued risk of HIV-1 acquisition [6].
2.4 Clinical DataWhile receiving PrEP, individuals were at a reduced risk of acquiring HIV-1 infection and those receiving CAB–LA could experience ISRs. Individuals who acquired HIV-1 infection incurred lifetime losses in life expectancy and QALYs and could potentially transmit HIV onwards. They could also acquire PrEP-related resistance mutations. Information on the clinical data used in the model to characterize these events is provided in the following sections.
2.4.1 HIV Incidence and PrEP EfficacyHIV incidence varied depending on the PrEP option (if any) an individual received. Base HIV incidence for MSM and TGW not receiving PrEP was taken from Mera et al. [26], as the HPTN 083 clinical trial did not include a placebo arm for ethical reasons. HIV incidence for MSM and TGW receiving CAB–LA or oral PrEP in the base-case analysis was taken from the HPTN 083 clinical trial [9]. In the sensitivity analyses, HIV incidence was adjusted to account for varying oral PrEP adherence rates [9, 24, 27] (see Online Resource for more information).
Base HIV incidence for cisgender women at risk has not been studied extensively in the USA, and the HPTN 084 clinical trial did not include a placebo arm for ethical reasons. Therefore, base HIV incidence was estimated from the number of cisgender women in the USA with and without a PrEP indication and available HIV-1 diagnosis rates (Online Resource Table S-1). HIV incidence for cisgender women receiving CAB–LA or FTC/TDF was taken from the HPTN 084 clinical trial [10]. All HIV incidence values used in the model are summarized in Table 2.
Table 2 Model inputs: clinical data2.4.2 Adverse Event IncidenceModeled individuals receiving CAB–LA could experience ISRs. Rates of ISR by severity were taken from the HPTN 083 (MSM and TGW) and HPTN 084 (cisgender women) clinical trials (Table 2). The model applied ISR events in the first year of the analysis, as ISRs that require management tend to occur early in CAB–LA use.
All other short-term adverse events were assumed to have similar, low incidence rates across all PrEP options, and long-term adverse events were assumed to be rare given the relatively short exposure to PrEP. Thus, adverse events beyond ISRs were not included in the model.
2.4.3 PrEP-Related Resistance MutationsIndividuals who acquired HIV-1 infection while receiving PrEP could develop PrEP-related resistance mutations and require different ARV treatment regimens than individuals without resistance. The incidence of PrEP-related resistance, measured as events per PY receiving PrEP, was 0.16% for individuals receiving CAB–LA [integrase strand transfer inhibitor (INSTI) resistance] and 0.19% for individuals receiving oral PrEP [nucleoside reverse transcriptase inhibitor (NRTI) resistance] [9, 28]. Data for all modeled individuals were taken from the HPTN 083 clinical trial because resistance data were not yet available from the HPTN 084 trial. Non-nucleoside reverse transcriptase inhibitor (NNRTI) resistance was not included in the model because none of the PrEP options include NNRTIs, so any observed NNRTI resistance after HIV acquisition must be transmitted rather than resistance associated with PrEP. Similarly, NRTI resistance was not included in the model for CAB–LA.
2.4.4 Secondary HIV InfectionsBy avoiding HIV-1 infection, individuals on PrEP avoid potential onward HIV transmission. On average, individuals who acquired HIV-1 infection in the model were estimated to transmit HIV to 0.80 others [29]. These secondary infections were generally assumed to occur in the acute phase of HIV disease progression, when viral load and risk of transmission are high before viral suppression is achieved via multiclass ARV treatment. This timing informed the discounting of associated costs, losses in life expectancy, and QALYs.
2.5 CostsOver time, modeled individuals incurred PrEP-related costs, including acquisition, administration, and monitoring costs, and could incur ISR management costs, lifetime HIV-related care costs, and PrEP-related resistance costs. Information about these costs is provided in the sections below.
2.5.1 PrEP-Related CostsPrEP acquisition costs were based on indicated dosing and unit costs (Table 3). Dosing was taken from the relevant product labels [3, 11, 30]. Unit costs were taken from Redbook using 2022 wholesale acquisition costs [31]. The cost of FTC/TDF was based on the lowest cost among the available generic options. The cost of CAB–LA was based on individuals receiving seven injections in year 1, according to the initiation dosing schedule, and six injections every year thereafter, based on every-2-month maintenance dosing [11]. Oral PrEP acquisition costs were adjusted to account for adherence observed in the HPTN 083 clinical trial, where the base-case analysis estimated an average of 3.95 doses taken each week by individuals receiving oral PrEP (Online Resource Table S-2). Conservatively, CAB–LA costs were based on indicated dosing and were not adjusted for adherence.
Table 3 Model inputs: PrEP-related costsAdministration costs for PrEP included the costs associated with injection administrations (CAB–LA) and routine physician visits (all PrEP) (Table 3). Monitoring costs for PrEP included the costs associated with laboratory tests recommended for individuals receiving PrEP in the clinical monitoring guidelines published by the CDC in 2021 [6] (Table 3 and Online Resource Table S-3).
2.5.2 ISR Management CostsManagement costs for ISRs were estimated by severity. Mild ISRs were assumed to require no medical management. Moderate ISRs were assumed to be managed with 800 mg of over-the-counter ibuprofen three times per day for 3 days after each injection in the first year of CAB–LA use, with a total cost per event of $4.51 [31]. Severe ISRs were assumed to require a physician visit [Current Procedural Terminology (CPT) code 99213] and the same ibuprofen regimen, with a total cost per event of $187.58 [32].
2.5.3 Lifetime HIV Management CostsIndividuals who acquired HIV-1 infection in the model incurred the cost of lifetime HIV-related care, including the cost of ARV treatment and ongoing monitoring. The total discounted lifetime cost of HIV-related care was taken from a study of incremental healthcare costs for commercially insured individuals living with HIV compared with individuals without HIV [33]. The cost reported in 2017 US dollars was inflated to $939,946 in 2022 US dollars [34] and was applied to all modeled primary and secondary infections at the time of HIV acquisition.
2.5.4 PrEP-Related Resistance Mutation CostsIn the model, individuals with PrEP-related resistance mutations were assumed to require different ARV treatment regimens than individuals without resistance for a period of time (Table 3). Individuals who acquired HIV-1 infection without PrEP-related resistance mutations were assumed to receive dolutegravir/lamivudine ($32,290 per year), the lowest cost INSTI-based single-tablet regimen currently recommended as an initial regimen for most people with HIV [31, 35]. Individuals with PrEP-related resistance mutations required more expensive first-line regimens. Specifically, individuals with INSTI resistance were assumed to receive darunavir/cobicistat/emtricitabine/tenofovir alafenamide ($49,489 per year) and individuals with NRTI resistance were assumed to receive dolutegravir + darunavir/cobicistat ($50,166 per year) [31]. Individuals with PrEP-related resistance mutations were assumed to remain on their more expensive regimens for the entirety of their first-line treatment. The average duration of first-line treatment was conservatively estimated to be 16.2 years, based on a 2011 study by Beck et al. [36]. Realistically, durations may now be shorter due to the availability of additional ARV options and the possibility of regimen optimization in the setting of viral suppression. Furthermore, PrEP-related resistance mutations may occur less frequently as HIV testing options continue to evolve.
2.6 Life Expectancy and QALY Losses Due to HIVIndividuals who acquired HIV-1 infection experienced losses in life expectancy and QALYs, with values estimated from published literature and publicly available life-expectancy data (Table 1). These losses were applied to all modeled primary and secondary infections. Individuals who did not acquire HIV-1 infection were assumed to have no losses in life expectancy or QALYs. Additionally, no utility or QALY decrements were applied while receiving PrEP because it was assumed that individuals choosing to receive PrEP view the choice positively, as benefits like decreased anxiety about acquiring HIV-1 infection may outweigh potential negative feelings on issues such as ISRs.
2.7 ValidationVarious validation processes were conducted to support confidence in the model and its outcomes. Specifically, the model structure, input parameter values, programming, and outcomes were validated according to the Assessment of the Validation Status of Health-Economic decision models (AdViSHE) tool [37]. Face-validity testing of the model structure, inputs, and outcomes was conducted by the authors and by clinical and health economic modeling experts external to the project team. Cross-validity testing was conducted by comparing the structure, inputs, and results of our model with those of several other models, as described in the Discussion section. The computer model in Excel was subjected to a predefined quality-check process that included extreme-value and other scenario testing as well as validation of all equations, code, input data, and results. The computer model was also independently assessed by a health economic modeling expert external to the project team and extensively reviewed and pressure tested by the authors. Finally, comprehensive sensitivity and scenario analyses were conducted to assess the impact of parameter uncertainty and alternate modeling assumptions and input parameter values on the model results, as described in the following sections.
2.8 Analyses2.8.1 Base-Case AnalysisThe base-case analysis assessed lifetime costs and health outcomes for individuals in the CAB–LA pathway versus the oral PrEP pathway (Fig. 1), assuming a 5-year duration of risk during which PrEP use could help prevent HIV-1 infection. Model outcomes included total costs by cost category, number of primary and secondary HIV-1 infections, life-years and QALYs lost due to HIV acquisition, and various ICERs (Table 4). All costs and health outcomes were discounted at 3% per year [21]. Willingness-to-pay thresholds in the USA commonly range between $50,000 and $300,000 per QALY gained [38, 39]. For this analysis, the CAB–LA pathway was considered cost-effective if the incremental cost per QALY gained was at or below $100,000 per QALY gained [38].
Table 4 Base-case analysis results2.8.2 Sensitivity AnalysesSensitivity analyses were conducted to assess the impact of parameter uncertainty on the cost-effectiveness results. In the one-way sensitivity analysis, input parameters were individually varied over their 95% confidence intervals (CIs). In the probabilistic sensitivity analysis, 10,000 iterations were conducted, where input parameter values were varied simultaneously and sampled from probability distributions via Monte Carlo simulation. The ranges and distributions used in these analyses were derived from published sources whenever possible and are described in additional detail in Online Resource Table S-4.
2.8.3 Scenario AnalysisA scenario analysis was conducted to assess the impact on the cost-effectiveness results of variations in PrEP use, the modeled population, and other key assumptions. Two real-world PrEP-use scenarios were examined to compare the CAB–LA pathway with no PrEP, as PrEP is still highly underutilized in the USA, and to test oral PrEP adherence observed in a real-world setting rather than in a clinical trial setting. Additional scenarios were conducted to assess the cost-effectiveness of the CAB–LA pathway in individual population subgroups that experience a disproportionate burden of new HIV-1 infections (i.e., MSM and TGW, African American/Black MSM, Hispanic MSM, White MSM, and cisgender women). For these subgroup analyses, HIV incidence for PrEP users was taken from HPTN 083 or HPTN 084 and, like the base-case analysis, base HIV incidence for MSM and TGW not receiving PrEP was taken from Mera et al. [26] and base HIV incidence for cisgender women was estimated from the number of cisgender women in the USA with and without a PrEP indication and available HIV-1 diagnosis rates (Online Resource Table S-1). The duration of HIV risk was varied in two scenarios to test the impact of shorter (2-year) and longer (10-year) durations of risk. Finally, scenarios were conducted to compare the CAB–LA pathway with a FTC/TAF pathway (where approved for use) and to assess variations in important PrEP use parameters, including persistence, switching, and monitoring. Specific scenarios tested are summarized in Table 5.
Table 5 Scenario analysis results
留言 (0)