
Remember me


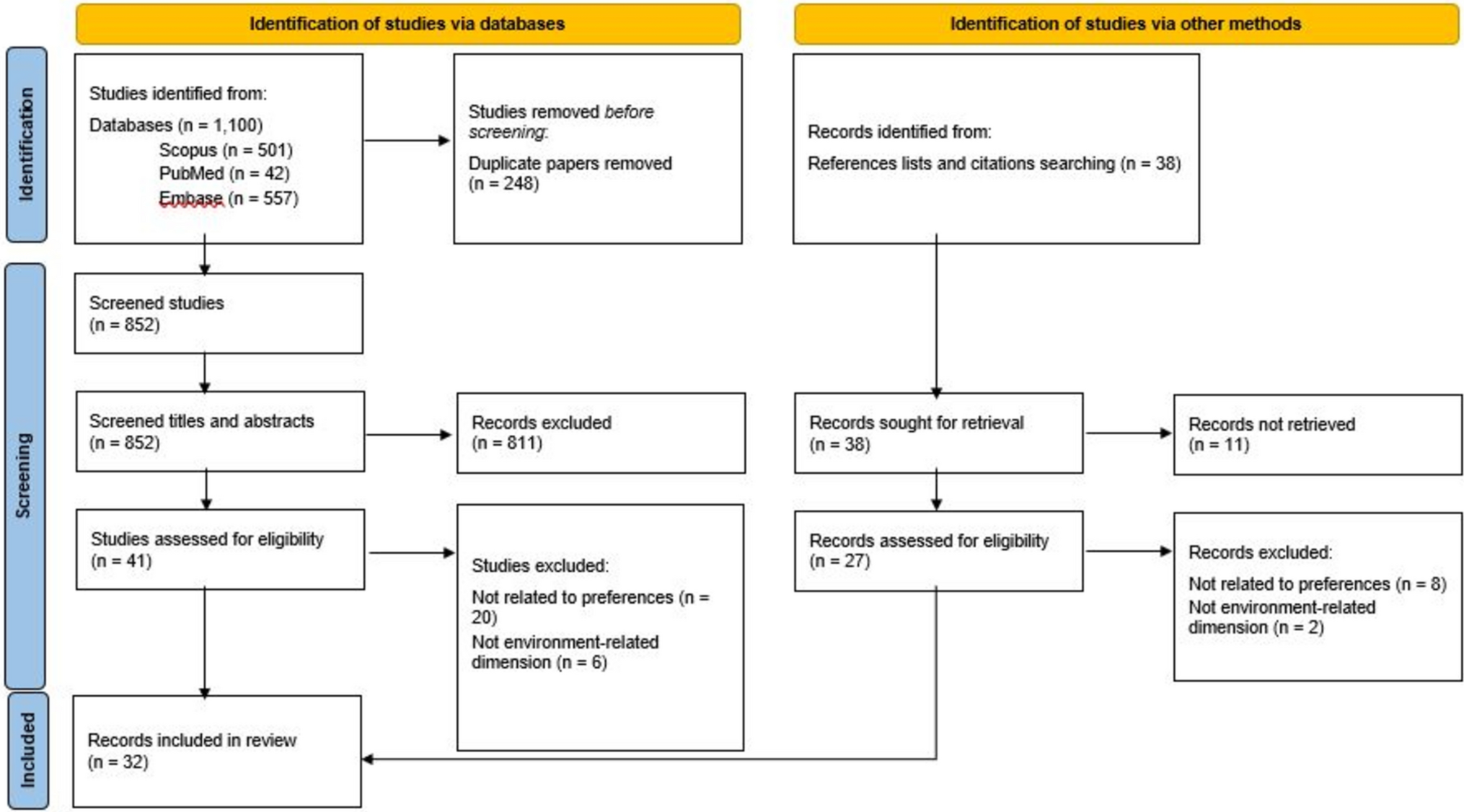
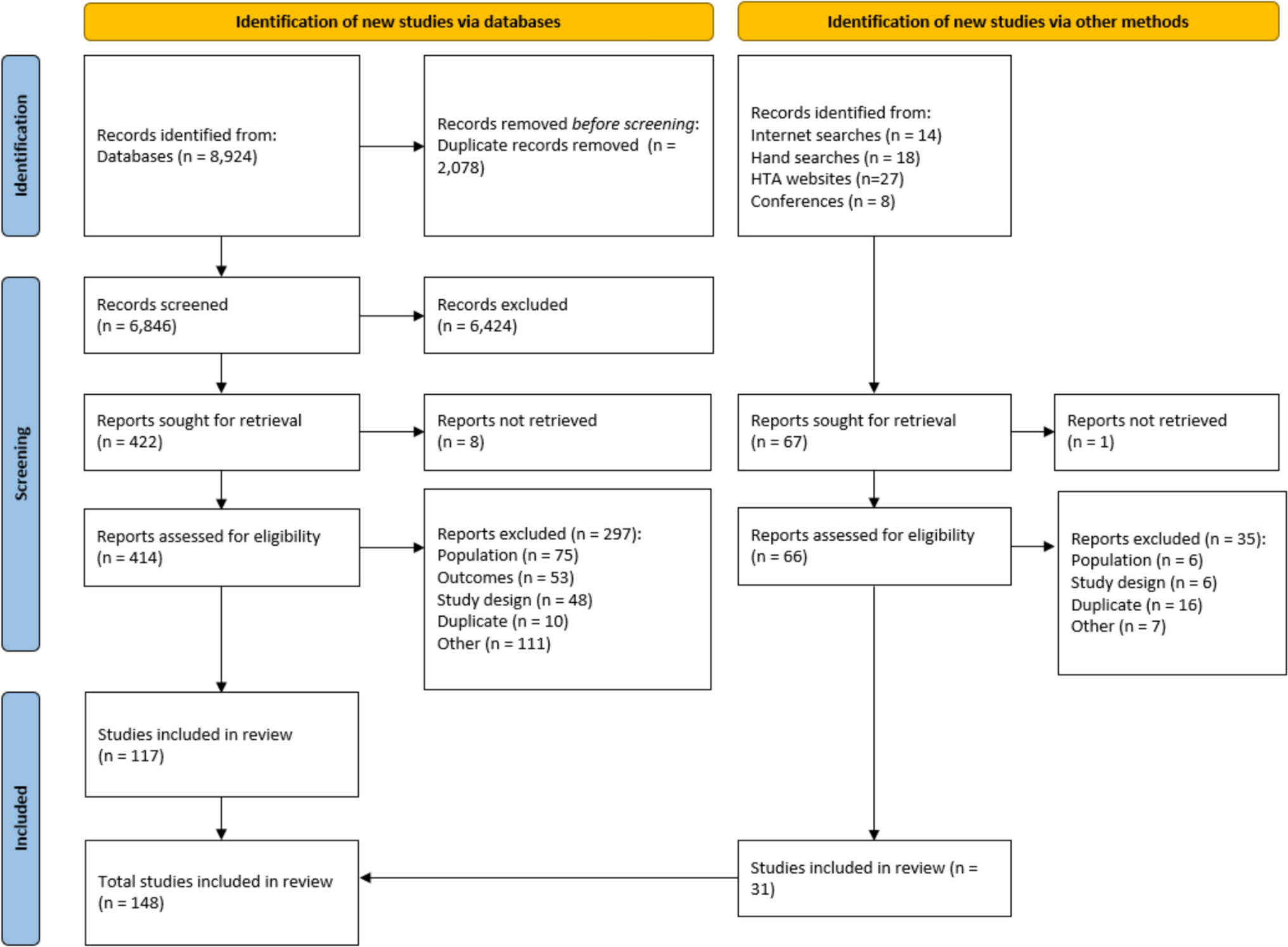
The search identified 1434 papers. After removing duplicates and documents that did not meet the inclusion criteria (1324 in total), and following a hand search of papers’ references, 117 articles were thoroughly read. Of those, 43 studies were ultimately included in the SLR (Fig. 2).
Fig. 2
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart
3.1 Risk of Bias AssessmentOnly one study was categorised as QC1 and three studies (6.98%) as QC2; 34 studies (79.07%) had scores of between 51 and 75 (QC3), and five studies (11.63%) scored 76 or more (QC4) [Table S3 of the ESM]) (Fig. 3). None of the studies was excluded because of the QC score, and therefore all are included in the final count.
Fig. 3
Number of studies in each Quality of Health Economic Studies (QHES) criterion interval. QC quality categories
In this SLR, none of the included studies was a “complete” economic evaluation (see Sect. 2.2), and therefore items Q12 and Q13 (8 and 7 points, respectively) were not mandatory in any of the included papers. Few scored points for Q12 [13, 14, 35,36,37,38] and only one scored points for Q13 [37] because it was proposed as a modelling study.
In the case of high scores related to data reporting (Fig. 1, grey bars), the highest number of studies falling into category QC4 were those in which the study objective was clearly reported (Q1) [reported by all except one study [39]], followed by those reporting the method of data abstraction (Q7) [reported by all except [2, 39,40,41,42,43]], those presenting conclusions/recommendations based on study results (Q15) [reported by all except one study [44]] and those disclosing the source of funding (Q16) [reported by all except [1, 3, 7, 35, 39, 40, 42, 45]].
With regard to items relating to study methodology quality (Fig. 1, blue bars), only one study rated as QC1 (Fig. 3, red bar), based on the low number of items reported (14). A subgroup analysis (Q4) was mentioned by only three studies [46], all of which rated as QC3; performance of incremental analysis between alternatives (Q6) was reported only by two studies [1], which rated as QC3 and QC4, respectively. Item Q4 (1 point) is virtually mandatory in the case of a randomised controlled trial, but few of the included studies were randomised controlled trials. Item Q6 has more weight in the QHES (6 points) and is mandatory in the case of complete economic evaluations, but in the case of cost studies there are no specific suggestions in any guidelines. The highest number of studies reporting items relating to methodology (QC4, Fig. 3, green bar) were those reporting the source of variable estimates (Q3) [reported in all studies except [39]]; analytic horizon, outcomes and justification of discount rate (when reported) (Q8) [reported in 37 studies, but not in [5, 15, 39, 40, 42, 45]]; methodology for measurement of costs and estimation of quantities/unit costs (Q9) [reported in 36 studies, but not in [2,3,4, 39, 40, 42, 43]]; primary outcome measure (Q10) [reported in 42 studies, but not in [40]]; and valid health outcomes measures/scales (Q11) [reported in all studies except [39]]. In all cases, the QHES score raised as the completeness of reporting in both domains (data report and study quality) increased (Table S6 of the ESM).
3.2 General Characteristics of StudiesThe data collected from the selected studies are from the databases created and the patients/caregivers interviewed from April 1993 [41] to September 2018 [47]. More than half of the studies (32 [69.77%]) were published from 2010 to 2022.
Most of the studies were conducted in the Americas, mainly in North America (the USA and Canada) [25 (58.14%)], and one in Latin America (Argentina). Seven were conducted in Europe (Finland, Germany, Spain, Italy, Greece and Ireland), four in the UK, four in Asia (India, China and Japan), one in Africa (Ethiopia) and one was multinational (USA, Ireland and the UK). The main characteristics of the included studies are summarised in Table S2 of the ESM.
More than half of the studies presented data on exclusively public healthcare programmes in the Americas, Asia and Europe (28 [65.12%]). Public-private services were mentioned in seven studies from Canada [9, 13, 15,16,17,18, 48], one from the USA [49], and one from the UK [47]; one study did not provide data on the health services provider [12]. Solely private care was the modality in two studies from the USA [2, 3], one from Greece [1], one from Italy [46] and one from Ethiopia [50]. Several studies (27 [62.79%]) reported data on patients receiving in-hospital care combined with different types of ambulatory care, and 37.20% (16 studies) reported mainly ambulatory or home-based care (Table 1).
Table 1 General characteristics of included studies (N = 43)Table 2 describes patients’ and caregivers’ main clinical and sociodemographic characteristics. All the studies included patients with cancer. Twenty-five studies (58.14%) reported cancer as a sole condition in the included patients, and 18 (41.86%) reported data on patients with cancer and patients with other non-oncologic diseases for which PC was provided. Out of all the studies with non-cancer patients requiring PC included as part of the sample, 12 (27.91%) had CHF and COPD, the main non-cancer conditions, and 7 (16.28%) reported dementia/AD. The severity of the conditions and the presence of comorbidities, illnesses unrelated to the one that led to the provision of PC, were also reported (for more details, see Table S2 of the ESM).
Table 2 Sociodemographic characteristics of patients and caregivers (N = 43)The study time frame (follow-up time) was variable, with range from up to a month in ten studies (23.81%) to at least 1 year in 18 studies (41.86%) and more than 2 years in one study [35]. Seven studies reported several follow-up and cost-measuring periods (i.e. repeated measures, related to the type of data analysis) [2, 5, 6, 15, 44, 49, 51]. Mean survival time after starting PC was reported in 12 (27.91%) of the studies, and median survival time was reported in seven studies (16.28%); in all cases, it was less than 1 year (Table 2).
All papers reported data on the patients’ characteristics, and ten (23.26%) reported data related to caregivers. Patient ethnicity was diverse and reported in nine studies; five were from the USA [2, 3, 7, 38, 52], one was from the UK [47], one was from China (Hong Kong) [45] and one was multinational (UK, Ireland, USA) [6]. The caregivers’ ethnicity was not mentioned in any paper.
The clinical professionals in the PC teams assigned to patients were diverse. Some had a specialist physician as a team leader and worked with other physicians, nurses, social workers and other healthcare personnel (e.g. various types of therapists). Others had nurses as team leaders [43]. There was no homogeneity in the composition of the teams (Table S4 of the ESM).
3.3 Cost MethodologyThirty-three studies (76.74%) were of costs only, ten (23.26%) were analyses of resource use (three cohort and six descriptive studies) and one used a decision model to estimate costs over longer time horizons [37] (Table 3). The predominant cost methodology was bottom-up (88.37%), and the main study design was retrospective (60.47%). The most common perspective for the analysis was that of the national health system (financer) (53.49%), and direct healthcare costs were the most commonly measured and evaluated costs. The follow-up period was reported in all 43 studies and was up to a year in 33 of them (76.74%).
Table 3 Methodological characteristics of studies (N = 43)All studies except for one [39] reported data on direct healthcare costs, and 12 (27,6%) reported data on direct non-healthcare costs [6, 9, 13,14,15,16,17,18, 47, 53,54,55]; 12 (27.91%) studies explored direct and indirect costs borne by patients and caregivers; three studies (6.99%) explored patients’ productivity losses [12, 45, 56] and ten (23.26%) caregivers’ productivity losses [9, 12, 13, 15,16,17,18, 45, 55, 56], all from a societal perspective (Table 3). Studies focusing on a societal perspective were mainly prospective.
Data on costs for a 1-year time horizon were collected through questionnaires administered to patients’ caregivers, using the opportunity costs method and collecting data on out-of-pocket expenditures, such as travel expenses, medications needed because of being a caregiver, and time and/or income loss. Only one study [17] measured the direct healthcare costs for carers. No study conducted a regression analysis to analyse the social and economic factors associated with caregivers’ income losses.
The time horizon and its linked data and discount rate were explicitly reported only in one study [57]. A regression analysis to define the factors that determine cost drivers was conducted in almost half of the studies (19 [44.19%]); a sensitivity analysis to test the robustness of the final result was conducted in six studies, but only one reported the type of analysis used (deterministic) [35] [details on regression variables in Table S5 of the ESM].
Twenty studies reported an increase in care intensity and, consequently, an increase in care costs in the end-of-life (EOL) period. Of these, 11 (25.63%) were studies made from the financer perspective (public or private) [4,
Comments (0)