BACKGROUND
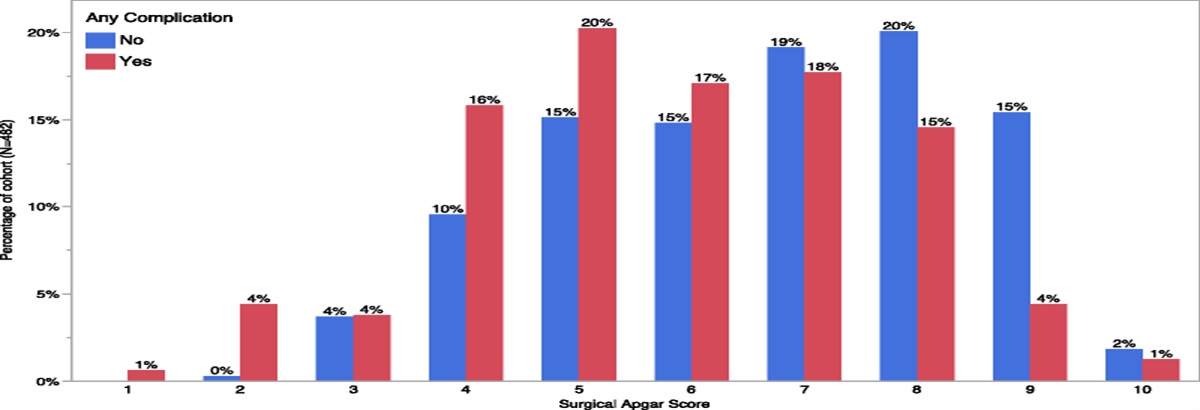
The Surgical Apgar Score (SAS) is a 10-point validated score comprised of three intraoperative variables (blood loss, lowest heart rate, and lowest mean arterial pressure). Lower scores are worse and predict major postoperative complications. The SAS has not been applied in emergency general surgery (EGS) but may help guide postoperative disposition. We hypothesize that SAS can predict complications in EGS patients undergoing a laparotomy.
METHODS
We performed a retrospective review of adult patients at a single, quaternary care center who underwent an exploratory laparotomy for EGS conditions within 6 hours of surgical consultation from 2015 to 2019. Patients were grouped by whether they experienced a postoperative complication (systemic, surgical, and/or death). Multivariable regression was performed to predict complications, accounting for SAS and other statistically significant variables between groups. Using this model, predicted probabilities of a complication were generated for each SAS.
RESULTS
The cohort comprised 482 patients: 32.8% (n = 158) experienced a complication, while 67.2% (n = 324) did not. Patients with complications were older, frailer, more often male, had worse SAS (6 vs. 7, p < 0.0001) and American Society of Anesthesiologists scores, and higher rates of perforated hollow viscus (p = 0.0003) and open abdomens (p < 0.0001). On multivariable regression, an increasing SAS independently predicted less complications (adjusted odds ratio, 0.85; 95% confidence interval, 0.75–0.96; p = 0.009). An SAS ≤4 was associated with a 49.2% predicted chance of complications, greater rates of septic shock (9.7% vs. 3%, p = 0.01), respiratory failure (20.5% vs. 10.8%, p = 0.02), and death (24.1% vs. 7.5%, p < 0.0001). An SAS ≤ 4 did not correlate with surgical complications (p = 0.1).
CONCLUSION
The SAS accurately predicts postoperative complications in EGS patients undergoing urgent laparotomy, with an SAS ≤ 4 identifying patients at risk for septic shock, respiratory failure, and mortality. This tool can aid in rapidly determining postoperative disposition and resource allocation.
LEVEL OF EVIDENCE
Therapeutic/Care Management; Level IV






Comments (0)