Definite or probable AT deficiency, PC deficiency and PS deficiency were observed in 80, 50, and 317 pregnancies, respectively, from 2014 to 2018 in Japan, with prevalence rates among total deliveries of 0.011%, 0.007%, 0.044%. In the peripartum period of current pregnancies, 27.5% of women with AT deficiency, 28.0% with PC deficiency and 13.2% with PS deficiency developed thrombosis. Of the thromboses that occurred, 92.3% occurred during pregnancy, and 62.8% occurred at less than 15 GW. Prophylactic anticoagulation significantly prevented the onset of peripartum thrombosis (p < 0.0001). There seem to have been few serious complications due to placental insufficiency other than growth restriction (SGA infants).
AT, PC and PS deficiency are the major types of thrombophilia in Japanese people [1, 5,6,7,8,9]. In this study, 4 cases of AT deficiency, 17 cases of PC deficiency and 126 cases of PS deficiency in the results of primary study [18] were excluded. Most of the cases that were excluded were those with low PS activity measured only during pregnancy, and those with plasma activity levels that did not meet the inclusion criteria (Table 1). If 100% of institutions had responded in this surveillance, it is estimated that there may have been up to 137 cases of AT deficiency, 85 of PC deficiency and 542 of PS deficiency during these 5 years. In other words, there could have been up to 27 cases of AT deficiency, 17 of PC deficiency and 108 of PS deficiency every year. National surveys by Ministry of Health, Labour and Welfare research groups and academic societies have indicated that there are about 2000 individuals with AT, PC, and PS deficiencies throughout Japan. The number of patients in whom these deficiencies newly develop annually is estimated to be less than 100 among neonates and infants, and about 500 among adults [19,20,21,22,23,24,25]. Thus, the estimated annual cases of pregnant women with hereditary thrombophilia in this study would seem to be reasonable. The prevalence of combined deficiencies in this survey was 3.2% (14/433). A nationwide survey in Japan conducted in 2009 revealed 12 patients with combined deficiencies among 183 patients with thrombophilia (combined AT and PC deficiencies; 4 cases, AT and PS deficiencies; 3 cases, PC and PS deficiencies; 5 cases), for a prevalence of 6.6% [26]. Furthermore, 5 cases of double mutations in PC and PS genes were reported among 55 patients with genetic mutations (9.1%) out of 173 Japanese patients with DVT [27]. Accordingly, the prevalence of combined deficiencies in cases of thrombophilia seems vary from 3 to 9% in Japan.
Three hundred and forty-six cases (77.4%) of thrombophilia (63.8% of AT deficiency, 76.0% of PC deficiency and 81.1% of PS deficiency) were diagnosed before the current pregnancies; however, the rates of gene analysis were low (30.0% of AT deficiency, 20.0% of PC deficiency and 3.5% of PS deficiency). Accordingly, the prevalence of type I or type II deficiency in each thrombophilia is not clear. Judging from activities and antigen levels, there seems to be more type I than type II in AT and PC deficiency, and more type II than type I in PS deficiency (Table 2). These tendencies would seem to be compatible with the fact that the PS gene polymorphism (PS p.K196E; type II deficiency) is seen in about 2% of the Japanese population [28,29,30,31].
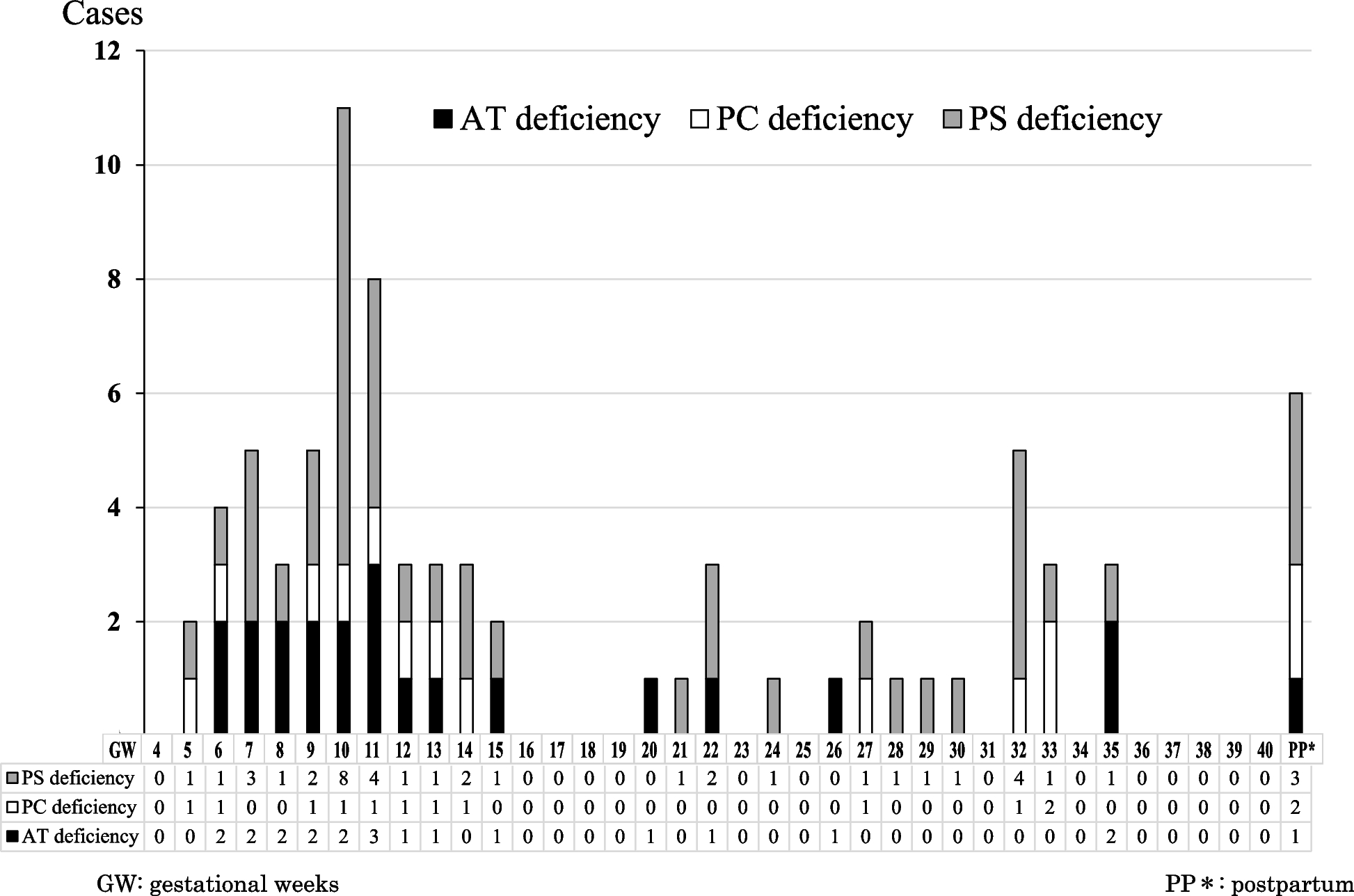
Hereditary thrombophilia is a syndrome in which severe thrombosis may develop before the age of 40 [1, 5,6,7,8,9]. Therefore, when a woman with thrombophilia becomes pregnant, thrombosis may develop during pregnancy or after delivery. Accordingly, prophylactic anticoagulation is recommended as long as thrombotic risks continue [1, 12,13,14]. In this survey, 27.5% of women with AT deficiency, 28.0% with PC deficiency and 13.2% with PS deficiency developed thrombosis in the peripartum period of the current pregnancy, showing significant differences compared to the control data for pregnant women (p < 0.0001) (Table 4). Pregnant women with AT and PC deficiency were more susceptible to thrombosis than those with PS deficiency (p < 0.01). Of the thromboses that occurred, 92.3% occurred during pregnancy, and 62.8% occurred at less than 15 GW (Fig. 1). As the earliest onset of thrombosis was 5 GW, prophylactic anticoagulation should be started as early as pregnancy is confirmed in women with previously diagnosed thrombophilia. Nine cases of thrombosis (5 cases of AT deficiency, 3 cases of PC deficiency and one case of PS deficiency) occurred despite prophylactic anticoagulation and in all of these cases there was a previous history and/or family history of thrombosis. On the other hand, 69 cases of thrombosis occurred in women who did not receive prophylactic anticoagulation, 25 of whom had a previous history and/or family history of thrombosis. Prophylactic anticoagulation significantly prevented the onset of peripartum thrombosis (p < 0.0001) (Table 5). Among 6 cases in which thrombosis developed postpartum, the latest occurrence was 3 months after delivery. Therefore, postpartum prophylactic anticoagulation for at least 3 months should be considered. The most commonly used prophylactic anticoagulation was 10,000 units/day of UFH. In the antepartum period, LDA alone without UFH, although it is not an anticoagulant therapy, was used in 90 cases (3 cases of AT deficiency, 6 cases of PC deficiency and 81 cases of PS deficiency) (Table 5). This seems to be the reason that prophylactic treatment is considered for RPL.
RPL is a state in which a woman has two or more consecutive abortions [32, 33]. As a hypercoagulable state is associated with RPL and sterility of unknown causes, screening for thrombophilia should perhaps be considered. A meta-analysis of 89 observational studies reported that women with FV Leiden mutation, prothrombin G20210A mutation, or PS deficiency had higher risks of RPL, and that AT or PC deficiencies were not associated with increased risk of RPL when compared with the reference population [34]. However, there is a large and contradictory literature on the association between maternal hereditary thrombophilia and RPL [32, 35,36,37,38,39,40,41,42,43,44,45]. Although the measurement of factor XII (FXII) is meaningful [43, 46], there was no significant difference in pregnant women with AT, PC, or PS deficiency [2]. With regard to decreased PS activity, an acquired decrease due to PS antibodies rather than to a genetic predisposition has been suggested [47]. In this survey, the rate of RPL was significantly higher in women with PS deficiency than in the controls (p < 0.0001) (Table 2). Considering the many published reports, although an association between low PS activity and RPL was demonstrated in this survey, it is unknown whether it is related to hereditary PS deficiency. In women with PC deficiency, the rate of RPL was significantly higher than in the controls in this survey (p < 0.0001). Although anecdotal evidence of high fetal loss has been reported in cases of severe PC deficiency [48], the reason for this association is unknown. A large-scale prospective study is needed.
In the current pregnancies in this study, obstetrical information such as age, body mass index, GW at delivery and preterm delivery were not significantly different compared to controls, but the rates of C-section, especially emergent C-section, in women with PC deficiency only were significantly higher (p < 0.05) than in controls. The reason why the rate of C-section in women with PC deficiency was 50% is unclear, but greater attention to the mode of delivery may be necessary in cases of PC deficiency (Table 3). Two cases of spontaneous abortion in women with AT deficiency (13 WG, 19 WG), one case in a woman with PC deficiency (19 GW) and one case in a woman with PS deficiency (20 GW) were observed. These data might suggest no association with RFL.
Fetal/neonatal risk for fetal demise, growth restriction, preterm birth, perinatal stroke, and cerebral palsy have been reported in infants with inherited thrombophiliac variants [16, 17]. In this survey, though there were significant increases in premature rupture of the membranes, placenta previa/accreta in women with PS deficiency and intrauterine growth restriction (SGA infants) in women with AT deficiency, there were no significant differences in the abovementioned maternal or fetal/neonatal complications due to placental insufficiency related to a hypercoagulable state compared to controls. On the contrary, gestational diabetes mellitus, atonic bleeding, breech presentation, multiple pregnancy, non-reassuring fetal status and neonatal asphyxia were significantly lower than in controls (Tables 3, 4 and 7).
In AT deficient pregnant women, administration of 1500 to 3000 units of AT concentrate (1.2 times the dosage with recombinant preparations) is recommended as supplemental therapy in addition to basic UFH, so that AT activity is at least 70% [1, 49, 50]. In this survey, prophylactic AT supplementation (the abovementioned recommended units) in patients with AT deficiency was more frequently performed compared to prophylactic anticoagulation both in the antepartum (54 cases vs. 42 cases) and intrapartum (48 cases vs. 19 cases) periods. Conversely, prophylactic anticoagulation was used more than AT supplementation (72 cases vs. 29 cases) in the postpartum period (Tables 5 and 6). Judging from the single case of postpartum thrombosis in a woman with AT deficiency, the obtained data seem reasonable. Accordingly, both prophylactic AT supplementation and prophylactic anticoagulation might be suggested in the antepartum period, AT supplementation rather than anticoagulation might be suggested in the intrapartum period, and anticoagulation rather than AT supplementation might be suggested in the postpartum period.
This study has several limitations. In this survey, pregnant women with hereditary thrombophilia were selected according to our inclusion and exclusion criteria. Pregnant women who did not meet the inclusion criteria, or who did meet the exclusion criteria, were excluded from this study. In particular, women with low PS activity measured only during pregnancy had to be excluded from the PS deficiency group. However, genetic screening was not performed in most cases. Although an association between low PS activity and RPL was demonstrated in this survey, it is unknown whether this is related to hereditary PS deficiency. The control data we used in this survey do not necessarily reflect the average Japanese data for delivery, because these data were collected from general hospitals and perinatal medical centers that tended to manage high-risk deliveries throughout Japan.






留言 (0)