
Remember me
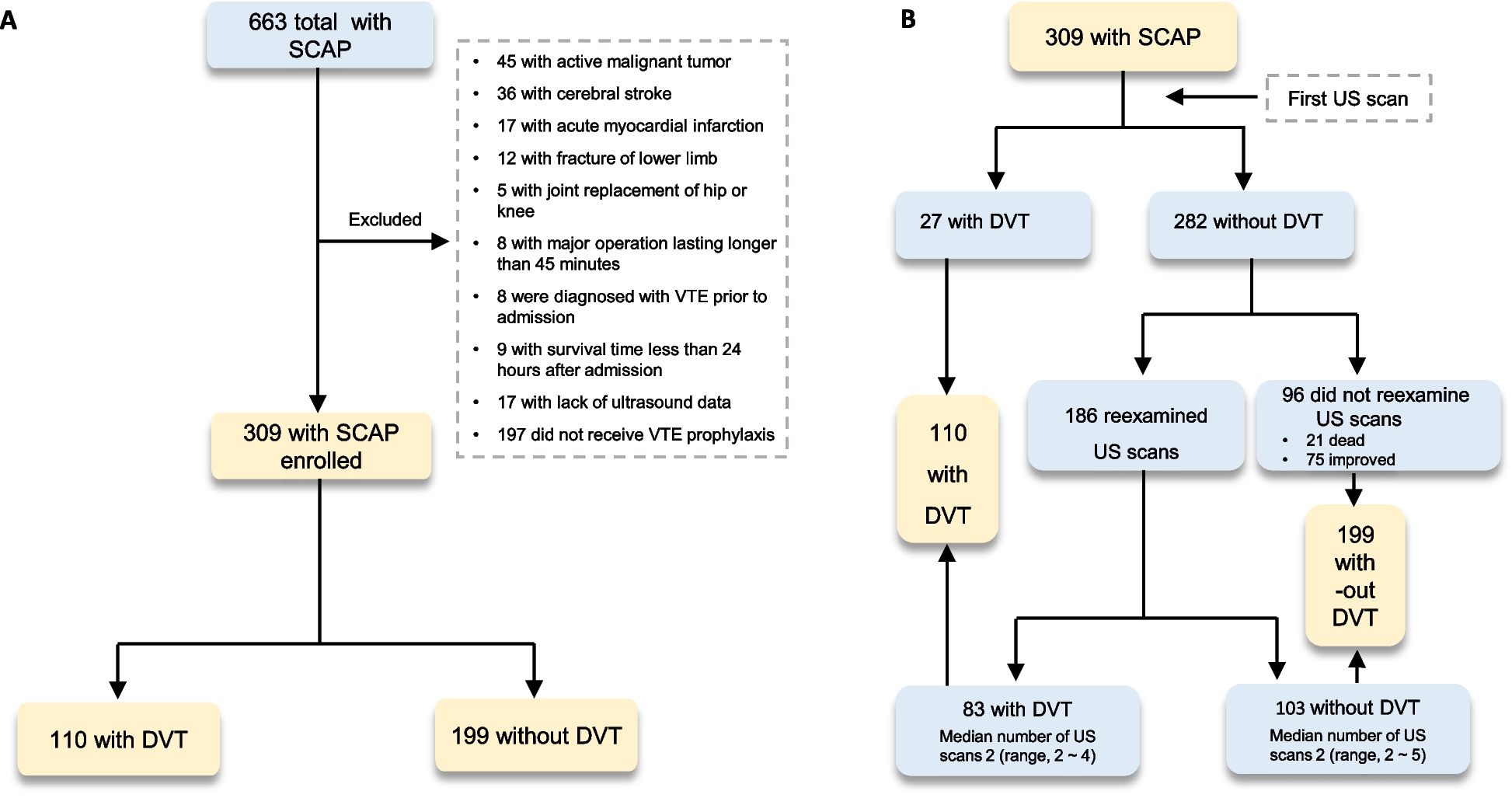







We identified 8534 patients who met the initial criteria for anemia associated with thrombocytopenia. Upon combining these patients with those showing signs of hemolysis, the cohort was reduced to 4081 patients. The classification process involved assessing the patients based on ICD-10 code diagnostics, medical history, sign of organ damage, and laboratory exams. From the analysis, we excluded patients with drug-induced hemolytic anemia (n = 1), autoimmune hemolytic anemia (n = 10), and those with a positive Coombs test (n = 8). Additionally, patients without evidence of organ damage were excluded (n = 1722). Consequently, the final classification yielded eight phenotypes of TMA, comprising a total of 2340 patients (Fig. 1).
Fig. 1
Flowchart Steps to Retrieve Patients with Thrombotic Microangiopathy (TMA)
Fig. 2
Thrombotic microangiopathy (TMA) by etiology in hospitalized patients
Secondary TMA was identified in 97.5% of the patients, whereas primary TMA, comprising TTP and aHUS cases, was found in 2.47% of the patients (Fig. 2). Among the cases of primary TMA, TTP was present in 1.79% of the patients, with a minimum platelet value of 10 [4,5,6,7,8,9,10,11,12,13,14,15,16]/µL, a median delta creatinine of 1.50 (1.24–1.81) mg/dl, and a mean arterial pressure (MAP) of 87 (78–100) mmHg. Plasmapheresis was administered to 40 out of 42 patients, with only 2 cases where it was not used due to concomitant leukemia. The aHUS patients represented 0.68% of the total TMA cases. Among the aHUS patients, the minimum platelet count was 82 (40–111)/µL, the delta creatinine was 3.11 (2.81–7.24) mg/dl, and the mean arterial pressure (MAP) was 107 (82–109) mmHg. Genetic analysis was performed on 7 aHUS patients, with pathogenic variants observed (2 cases related to CFH, 2 related to CFHR1-CFHR3, 1 to CFB, 1 to CFI, and 1 to C3). Furthermore, 14 aHUS patients received treatment with eculizumab.
Among the secondary TMA etiologies, the most frequent were infectious cases (44.62%), with 9.7% of those being attributed to COVID-19. Malignancy accounted for 26.84% of cases, making it the second most common cause. The third most prevalent etiology was TMA secondary to transplantation, representing 16.75% of the cases. TMA related to pregnancy was present in 6.71%, with eclampsia/HELLP syndrome accounting for 43% of those cases. Patients with STEC-HUS comprised 1.67% of the cohort and were confirmed to have positive stool cultures for Escherichia Coli. Malignant hypertension accounted for 0.90% of the cases and was confirmed through typical fundoscopic findings, including disc edema, arteriolar constriction, peripapillary flame-shaped hemorrhages, and cotton-wool spots.
In comparison to the other groups, patients with TTP, pregnancy-related TMA, and aHUS were found to have a lower age (Table 1; Fig. 3A, supplementary Table 1). The presence of severe hypertension and cardiovascular disease was more frequent in malignant hypertension. Kidney disease was more commonly found in patients with TMA related to transplantation and malignant hypertension. On the other hand, liver disease was more frequently observed in cases of infectious-related TMA (Table 1). The mean arterial pressure was higher in the groups of patients with malignant hypertension, pregnancy-related TMA, transplant-related TMA, and aHUS (as shown in Fig. 3B and supplementary Table 2). Patients with a transplant had higher levels of delta creatinine compared to the other groups (as shown in supplementary Tables 3 and Fig. 4). Patients with TTP had lower levels of platelets compared to the other groups (as shown in supplementary Table 4). Furthermore, patients with malignancy and infectious-related TMA had higher values of prothrombin time, AST (aspartate aminotransferase) values, and total bilirubin (as demonstrated in Fig. 5). Detailed multiple comparisons between the examinations and TMA classifications can be found in supplementary Tables 4–9. The infectious etiologies associated with TMA were detailed in Supplementary Table 10.
Table 1 Baseline characteristics, comorbidities, and associated conditions stratified by thrombotic microangiopathy (TMA) in hospitalized patientsFig. 3
A. Age in patients stratified by thrombotic microangiopathy (TMA). B. Mean Arterial Pressure (MAP) in patients stratified by thrombotic microangiopathy (TMA).
Fig. 4
Laboratory exams (delta creatinine, LDH, Hemoglobin, platelets) in patients stratified by thrombotic microangiopathy (TMA). (Values in log10 scale)
Fig. 5
Laboratory exams (AST, Bilirubin, TP and haptoglobin) in patients stratified by thrombotic microangiopathy (TMA). (Values in log10 scale)
Predictive modelWe initially employed a Lasso regression to select all available predictors. This process resulted in a reduced number of predictors used to fit the model, including the following variables: age, delta creatinine, maximum LDH, minimum platelets, minimum hemoglobin, maximum AST, maximum total bilirubin, maximum prothrombin time, maximum partial thromboplastin time, presence of hypertension, presence of cardiovascular disease, presence of kidney disease, presence of liver disease, presence of autoimmune disease, active transplant, active malignancy, active pregnancy, presence of infection, active COVID infection, and mean arterial pressure.
We applied three different models, namely Xgboost, LightGBM, and Lasso regression, to the train set comprising 1754 samples. The performance metrics were then evaluated on the test set containing 586 samples. Among the models, LightGBM demonstrated superior performance, as indicated in Table 2. The LightGBM model achieved an accuracy of 0.979 and a multiclass ROC-AUC of 0.966 (link to the predictive model: https://nephrologymodels.shinyapps.io/TMApred/).
Table 2 Performance metrics of machine learning model in the test set to predict thrombotic microangiopathy (TMA) in hospitalized patientsThe predictions showed higher accuracy in cases of infectious-related TMA, malignancy, malignant hypertension, pregnancy-related TMA, transplant-related TMA, and TTP. However, the predictions had lower confidence in cases of aHUS and STEC-HUS, as shown in Fig. 6.
Fig. 6
ROC AUC of LightGBM model to predict thrombotic microangiopathy (TMA) stratified by the predictions in each class
The strongest predictors associated with TMA classification were identified as follows: presence of infection, presence of hypertensive emergency, active transplant, age, active malignancy, active pregnancy, minimum platelets, delta creatinine, kidney disease, and active transplant, as shown in Fig. 7.
Fig. 7
Importance of Predictors of the LightGBM model to predict thrombotic microangiopathy (TMA).
Practical examples of TMA-INSIGHT predictionWe provided examples of eight patients, including their clinical characteristics and biochemical data. The TMA-INSIGHT retrieved the class probability for each patient in their respective classes. For more details on these examples, please refer to the Supplementary Practical Examples and Tables 10 and 11.
External validationWe conducted an external validation of the TMA-INSIGHT score using a Brazilian cohort of aHUS patients [12]. This cohort compromised 75 aHUS cases, including adults (53.4%) and children with a median age of 20.7 years [12]. Within this cohort, we were able to obtain clinical and biochemical data to validate the TMA-INSIGHT score. The results showed that the majority of the cases were corrected classified as aHUS (n = 44, 59%), followed by transplant-associated cases (n = 12, 16%), malignant hypertension (n = 8, 11%), pregnancy-related (n = 5, 6.7%), STEC-HUS (n = 3, 4%), and TTP (n = 3, 4%). Both infectious-related and malignancy-related cases demonstrated a zero probability. The model exhibited a multiclass accuracy of 0.586, sensitivity of 0.586, and specificity of 0.941.
Comments (0)