
記住我
The focus of this article is the participation of the biobank in the inception cohort of the SwiSCI study. The SwiSCI biobank provides a framework for conducting research projects nested within the SwiSCI cohort study. Detailed information on the SwiSCI study design and collected data can be found elsewhere [8, 9]. In brief, SwiSCI is established as prospective cohort study in collaboration between four major rehabilitation centers across Switzerland that serve as regional catchment areas for individuals requiring specialized therapy for SCI. Individuals with an SCI attributable to a congenital condition, neurodegenerative disorder, or Guillain–Barré syndrome, or who had a new SCI in the context of palliative care, were not invited to participate. A wide range of demographic, biopsychosocial, clinical parameters and biological samples from persons newly diagnosed with traumatic (TSCI) or non-traumatic (NTSCI) SCI receiving primary specialized rehabilitation were prospectively collected.
Data acquisition commenced on 1st May 2013 for inpatients and was extended to outpatient settings starting 1st August 2016. Data are collected at four distinct post-diagnosis time-points: T1 (28 days, range: 16–40 days), T2 (84 days, range: 70–98 days), T3 (168 days, range: 150–186 days), and T4 (0–15 days prior to discharge). Among the rehabilitation centers, three contribute to routine SwiSCI biobank sampling, while the fourth—University Hospital Balgrist—engages in project-specific biosampling.
Blood and urine serve as the primary biospecimens earmarked for long-term storage due to their minimally invasive (blood) or non-invasive (urine) collection methods. This aligns well with routine clinical practices, allowing for easy integration of biobank biosampling. Other clinically pertinent data such as MRI findings may be incorporated into future studies as they are stored in a centralized clinical database.
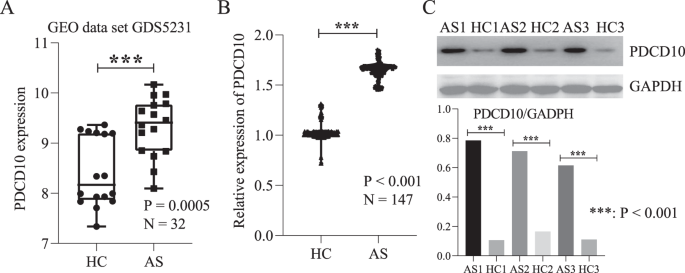
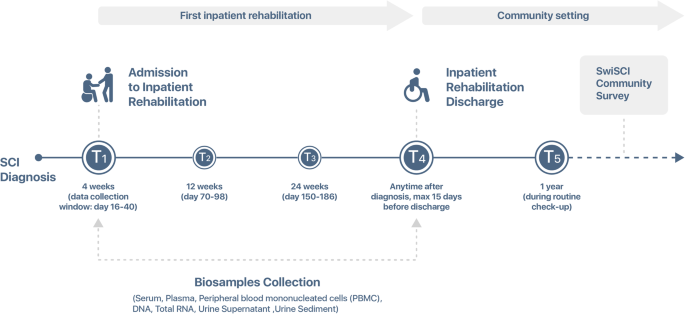
Biobank sampling is conducted at time points T1 (admission to rehabilitation) and T4 (discharge from rehabilitation), Fig. 1. These time points are consistent with the general SwiSCI assessment schedule. Upon consenting to participate in the SwiSCI study, patients undergo routine blood sampling for cardiovascular risk factors at these time-points to minimize patient burden.
Fig. 1: Schematic representation of longitudinal data and biosample collection in the SwiSCI Inception Cohort.
This figure delineates the timeline and specific time points (T1 to T4) at which both clinical data and biological samples were collected within the context of the SwiSCI inception cohort study.
Biobank sampling was initiated on 27th June 2016 in the SPZ in Nottwil, followed by REHAB Basel Klinik für Neurorehabilitation und Paraplegiologie and CRR Suva (Clinique romande de réadaptation) on 23rd August 2018 and 15th January 2019. Funding for the SwiSCI biobank is provided by the Swiss Paraplegic Foundation.
The SwiSCI biobank services as infrastructureAdditionally, to the core use as a SwiSCI biobank, in 2021, the SwiSCI biobank Infrastructure was founded and also certified by Swiss Biobanking Platform (SBP), allowing to collect, process and store biosamples from other studies, connected or not to SwiSCI. At the moment, the SwiSCI biobank Infrastructure collects or has collected biosamples for three additional studies: UROVAXOM, TASCI and Athletic-probiotic study. Serum, plasma, peripheral blood mononuclear cells (PBMC), RNA, DNA, urine and urinary microbiome biosamples are being collected within the UROVAXOM study, which is a pilot clinical trial that aims to explore the role of immunomodulation for primary prevention of urinary tract infections in patients with SCI [10]. Within the TASCI study, a randomized prospective clinical trial aimed to explore the efficacy of transcutaneous tibial nerve stimulation in preventing neurogenic detrusor overactivity, serum, plasma, PBMC, RNA, DNA, urine, urinary and gut microbiome biosamples are prospectively processed and stored [11]. Finally, we have recently finalized collection of serum, plasma and gut microbiome biosamples within the pilot randomized clinical trial which aimed to assess the feasibility of probiotic and prebiotic intervention in athletes with SCI (the Athletic study) [12].
Ethics, governance and management of the biobankThe SwiSCI biobank ethical approval was given on 2nd November 2015 by the Ethikkommission Nordwest- und Zentralschweiz (EKNZ). The biobank has a clearly defined governance and organizational structure. The head of the biobank is responsible for strategic management and collaborations and has the overall responsibility for operating the biobank. Administration and operational management are done by the operational manager who ensures the day-to-day functioning, compliance to the regulations and supervision of technical assistants.
The SwiSCl Study Center coordinates the research assistants in the participating centers. Responsibility of the anonymisation management is with the clinics. The key fiduciary manages the key according to a defined procedure, de-coupling privacy-related information from the corresponding downstream samples and data.
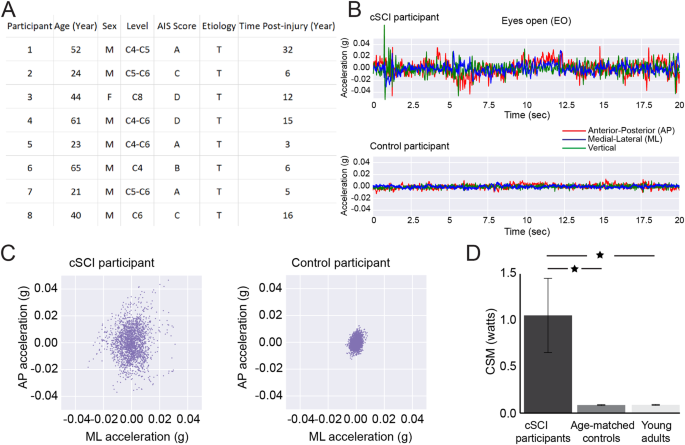
The SwiSCI study is overall monitored and controlled by the SwiSCI steering committee. The biobank controllers are responsible for the monitoring and coordination of the SwiSCI biobank. The head of the biobank reports to the biobank controllers and the steering committee. An organigram of the biobank shows the responsibilities and involved parties (Fig. 2).
Fig. 2: Organizational structure of the SwiSCI biobank.
The organigram illustrates the hierarchical and functional architecture of the SwiSCI biobank, showcasing the relationship between various stakeholders, departments, and processes integral to its operations.
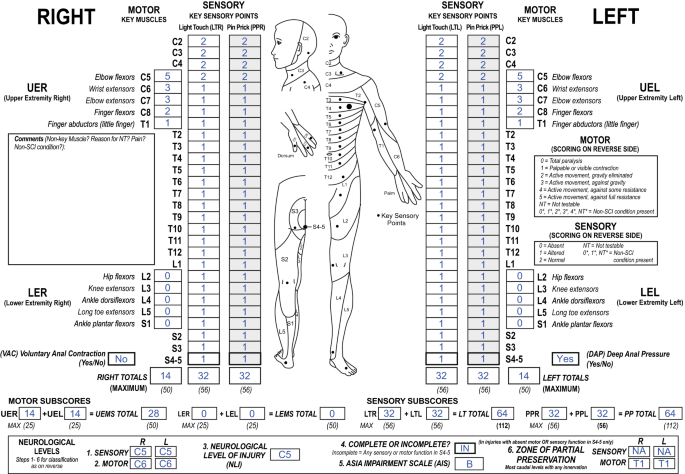
Recruitment procedurePotential study participants are recruited at SwiSCI centers by trained research assistants. The informed consent procedure is standardized between the centers and is performed just before or during early rehabilitation. No consent is collected in emergency contexts such as the acute surgery phase but afterwards. Consent can be withdrawn at any time. In the event of withdrawal, all biosamples and samples belonging to that participant are to be destroyed. The neurological status of the participants was described using theASIA/ISCoS International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) [13].
Biospecimen collectionAll reception and processing steps are formalized in standard operating procedures (SOPs). Peripheral whole blood is collected by trained clinical staff. The phlebotomy procedure uses a butterfly clip (BD) and is standardized across the participating centers. Peripheral whole blood is collected in several formats; (a) monovettes that contain silica clotting factor (Sarstedt), monovettes containing K3 EDTA (Sarstedt), and PAXGene RNA stabilization vacutainers (BD). Silica clotted blood is processed into serum. K3 EDTA blood processed into plasma, genomic DNA (gDNA) and PBMC. PAXGene tubes are processed into total RNA (including miRNA). Urine is collected in standard urine monovettes (Sarstedt). Urine is centrifuged, the supernatant is sterile filtered and stored as urine while the pellet is stored as urine sediment. For the TASCI study, immediately after collection the urine is kept on ice until processing. As the TASCI study requires urine purines, 2 mL of the collected urine is boiled shortly. Feces (for TASCI and Athletic study) are collected in gut microbiome DNA collection tubes (OMNIGENE). For more details see Table 1.
Table 1 Overview of currently available biosamples.The research assistants in the centers retrieve the monovettes and vacutainers from the clinical wards and remove any identifying information before re-labeling with anonymized IDs (SwiSCI ID or TASCI ID); Infrastructure projects follow the instruction of the study principal investigator (PI). The primary biomaterials collected in SPZ Nottwil are directly handed over to the biobank staff. Biospecimen from REHAB Basel are shipped by express courier to Nottwil and processed/stored by SwiSCI biobank. CRR processes the biospecimen on their own using the same SOPs used in the SwiSCI biobank; frozen samples are shipped to Nottwil on dry ice.
After arrival, SwiSCI biobank personnel assess the fresh biospecimen sets from SPZ or REHAB and uses time stamps (i.e. on collection times, arriving times), volumes and issues among other parameters on sample summary and for REHAB reception sheets. The arrival of the already processed and frozen samples from CRR is also documented on a reception form.
Biosamples processingApart from the SOP for PBMC processing and isolation, feces collection and urine purine storage, all SOPs are derived from and comply with CEN/TS standards for Isolated RNA (CEN/TS 16835-1), Isolated DNA (CEN/TS 16835-2) and urine, venous blood serum and plasma (CEN/TS 16945).
Collection volumes, storage temperatures and storage volumes/amounts can be found in Table 1. For storage, four different types of Azenta Life Sciences tubes are used: 1.9 mL tri-coded tube, 48-format, external thread (with screw cap), with a maximal working volume of 1.9 mL; 1.0 ml tri-coded tube, 96-format, external thread (with screw cap), with a maximal working volume of 1.0 mL; 0.5 mL tri-coded tube, 96-format, external thread (with screw cap), with a maximal working volume of 0.52 mL; and 0.26 mL dual-coded tube, 96-format, external thread (with screw cap), with a maximal working volume of 0.26 mL. A camera-based reader for SBS racks is used for scanning the aliquots into the database and later for fast identification of the SBS-format racked, 2D-coded tubes. The Biobank is managed with the FreezerPro® Sample Management System (Azenta US, Inc).
Detailed SOPs are created for each biobanking process. In brief, after clotting for 30 min at room temperature (RT), the serum monovettes are centrifuged at 1500 x g for 15 min, acceleration and brake speed at 9. The supernatant is aliquoted and stored at −80°C. The urine monovettes are centrifuged at 3000 x g for 5 min at 4°C. The supernatant is pipetted down to the 1 mL mark and pooled before filtration through a 0.22 µm membrane. The remaining 1 mL fractions in the monovettes are vortexed and pooled to generate the urine sediment fraction. The filtered urine supernatant is aliquoted, while the urine sediment is stored as a separate aliquot. All urine fractions are frozen at −80°C. For DNA extraction, 1 mL of K3 EDTA blood is taken directly from one monovettes. Genomic DNA is isolated using the GeneJet kit according to the manufacturer’s instructions and aliquots are stored at −80°C.
The rest of the K3 EDTA blood is gently decanted into a Leukosep tube containing 15.5 mL Lympholyte® Cell Separation density gradient centrifugation media (CEDARLANE). The tube is centrifuged for 20 min at 800 x g, acceleration speed 4, brake speed 0. The plasma layer is pipetted down to approximately 1 cm above the buffy coat, and aliquots are stored at −80°C. The buffy coat is gently aspirated, mixed with complete RPMI (cRPMI) and pelleted at 300 x g for 10 min (acceleration and brake speed 9). The pellet is resuspended in 10 mL cRPMI. Cells are counted using colter method (Scepter Millipore) in addition to a viability assessment with 0.4% Trypan Blue. After a centrifugation at 300 x g for 10 min (acceleration and brake speed 9), the pellet is resuspended in ice cold FBS to achieve a concentration of 10 × 106 PBMC/mL. 2.5 × 105 cells are assayed in triplicate in an alamar blue metabolic assay to establish metabolic activity. The remaining PBMC are diluted to 5 × 106 PBMC/mL with drop by drop addition of ice cold 2X freezing media composed of 20% dimethyl sulfoxide (DMSO) and 80% cRPMI. Cells are either aliquoted in 500 µL (2.5 × 106 PBMC) or 1 mL (5.0 × 106 PBMC) samples. Mr. Frosty containers for rate limited cooling at −1°C/min are used in a −80 °C freezer before storing at −150 °C freezer.
RNA is isolated from 5 mL of peripheral whole blood stabilized in PAXGene RNA vacutainers (BD), using the miRNA isolation kit (Qiagen) according to the manufacturer’s instructions and aliquots are stored at −80 °C. Feces are collected in fecal stabilization tubes (OMNIGENE), homogenized, stored at −80 °C.
Sample processing has to stick exactly to the previously validated and approved SOPs. Every deviation can cause variance in later experiments and therefore has to be noted on the work lists and in the database to be trackable. Time stamps and involved persons have to be noted. SOP version changes are recorded as well as the information which version was used per patient and donation time point.
Data managementThe SwiSCI data derived from patients is coded by an independent unique identifier with a neutral number from the point of view of the researcher. SwiSCI Study and the SwiSCI biobank data are kept in secure web-based SQL database, which is protected by passwords and have daily back-up. The SwiSCI study center also tracks changes to their databases and the identity of the person who accesses them. Biosample handling is performed only with encrypted samples, which are transferred for processing and cryopreservation the SwiSCI biobank according to validated workflows and standard operational procedures. Researchers can apply for SwiSCI data and samples by submitting a research proposal to the Study Center (swisci.research@paraplegie.ch) that undergoes an internal peer review process. Upon approval of the research proposal, pseudonymized data are provided to researchers for analysis. Samples for analysis are provided after an additional approval by the responsible ethics committee.
Statistical analysesThis paper reports on data collected in the inpatient setting during the period between 27th June 2016 and 19th October 2023. We summarized the baseline characteristics of our study population using mean (and standard error), median (and interquartile range) or counts (and percentages) as applicable. We used the Shapiro-Wilk test to determine the normality of the distribution of SwiSCI study participants characteristics. Kruskal-Wallis signed-rank test or Chi-squared test were used to determine differences in demographic and clinical profiles between SwiSCI study participants collected through three recruitment centers (SPZ, REHAB and CRR). All analyses were performed using Stata 16.1 (StataCorp LLC, College Station, TX) for Windows. All computations were done using two-tailed tests, and a p-value of <0.05 was considered statistically significant.
留言 (0)