
記住我
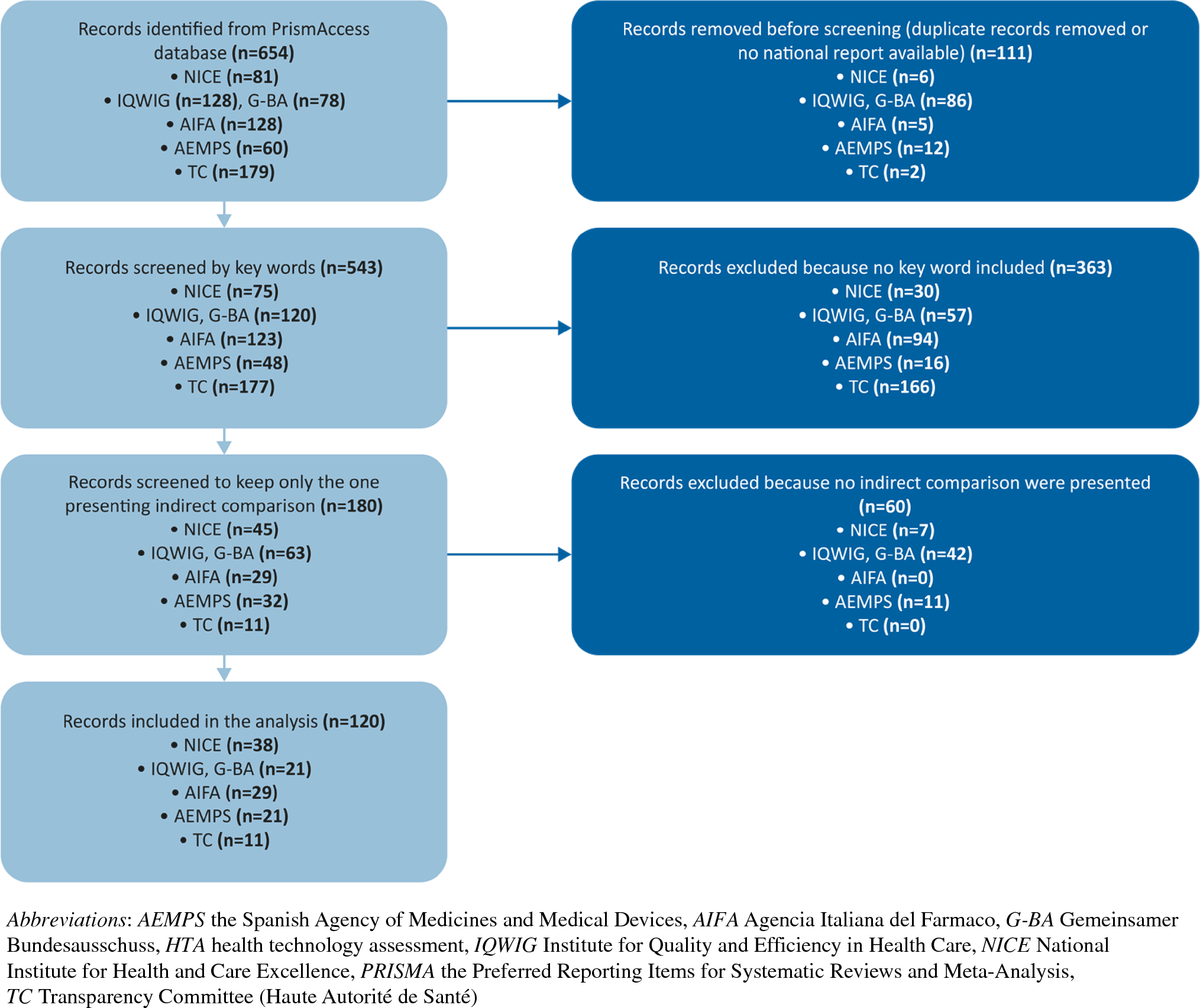

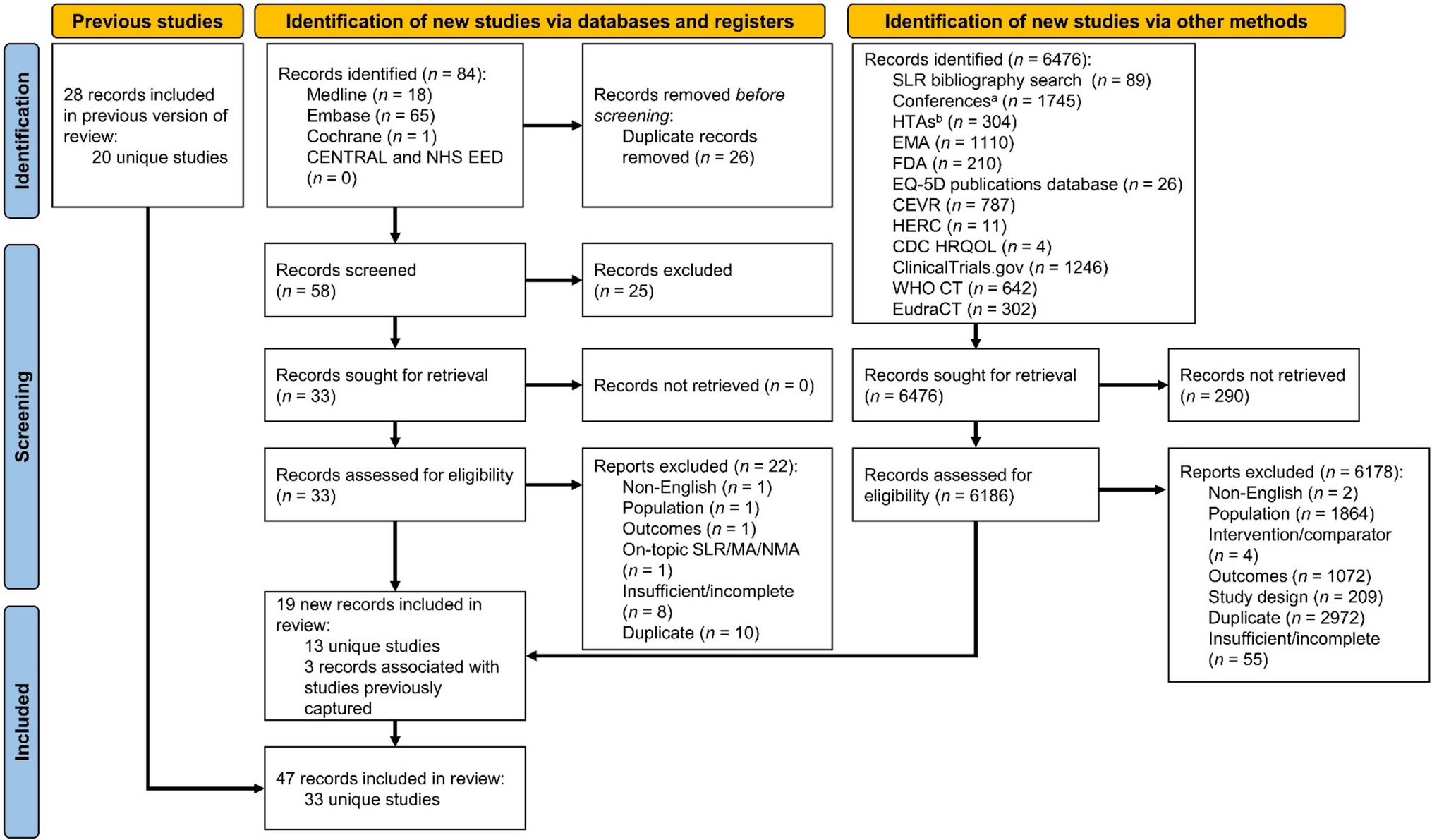

The initial SLR identified 1072 records and an additional 84 when updated (Fig. 1 and Supplementary Fig. S1). The initial gray literature search identified 8244 additional records for consideration and 6476 more when updated. After removing duplicates, screening, and searching reference lists and Supplementary Material, a total of 33 unique studies reporting HRQOL outcomes were included in the qualitative synthesis. Studies included in this analysis that reported HRQOL measures or health state utility values are summarized in Supplementary Table S4.
Fig. 1
PRISMA flow diagram. CDC Centers for Disease Control and Prevention; CEVR Center for Evaluation of Value and Risk in Health; EMA European Medicines Agency; Embase Excerpta Medica dataBASE; EQ-5D EuroQol 5-dimensional; EudraCT European Union Drug Regulating Authorities Clinical Trials Database; FDA United States Food and Drug Administration; HERC Health Economics Research Centre; HRQOL health-related quality of life; HTA health technology assessment; MA meta-analysis; MEDLINE Medical Literature Analysis and Retrieval System Online; NMA network meta-analysis; NHS EED National Health Service Economic Evaluation Database; PRISMA Preferred Reporting Items for Systematic reviews and Meta-Analyses; SLR systematic literature review; WHO CT World Health Organization Clinical Trials. aConferences searched included American Association for Cancer Research (n = 426), American Society of Clinical Oncology (n = 313), American Society of Hematology (n = 745), European Hematology Association (n = 178), European Society for Medical Oncology (n = 33), International Society for Pharmacoeconomics and Outcomes Research (n = 50). bSources of HTAs searched included Canadian Agency for Drugs and Technologies in Health (n = 22), Health Technology Assessment International (n = 0), Institut National d’Excellence en Santé et en Services Sociaux (n = 64), National Institute for Health and Care Excellence (n = 73), Pharmaceutical Benefits Advisory Committee (n = 13), and Scottish Medicines Consortium (n = 132)
3.2 HRQOLSeven studies were identified that assessed and reported disease-specific HRQOL measures (Table 2).
Table 2 Overview of included studies on HRQOL measures3.2.1 CAR T Cell TherapiesThree studies reported HRQOL data in patients with LBCL treated with CAR T cell therapies, including lisocabtagene maraleucel (liso-cel; n = 186 [17] and 184 [18] evaluable patients) and tisagenlecleucel (n = 108 [19]). In the phase 1, seamless design, single-arm trial of liso-cel (TRANSCEND NHL 001 [17]), the EORTC QLQ-C30 global health status instrument was used to assess HRQOL in patients with third-line or later LBCL who received liso-cel [35,36,37]. Baseline HRQOL scores improved by + 17.5 points at the month-12 follow-up after treatment.
The TRANSFORM trial [18] used the FACT-Lym subscale and EORTC QLQ-C30 to evaluate HRQOL in patients with LBCL treated with liso-cel or standard of care (SOC; platinum-based immunochemotherapy followed by carmustine, etoposide, cytarabine, and melphalan, and autologous HSCT in responders) as second-line therapy [18]. Mean change at day 126 (2 months after treatment) from baseline was reported. Improvements in mean scores were observed for both instruments for liso-cel and SOC. For liso–cel–treated patients, the mean [95% confidence interval (CI)] FACT-Lym increase was + 1.48 (0.30‒3.26) and the mean EORTC QLQ-C30 increase was + 3.08 (− 1.83 to 7.99); for SOC-treated patients, the mean (95% CI) FACT-Lym increase was + 1.63 (0.41‒3.68) and the mean (95% CI) EORTC QLQ-C30 increase was + 0.04 (− 5.24 to 5.31).
In the JULIET trial, change in HRQOL in patients with LBCL after treatment with tisagenlecleucel in the third-line or later setting was measured using the FACT-G, FACT-Lym, and SF-36 instruments [19]. HRQOL improved from baseline to 18-month follow-up across all instrument subscales, with mean change scores ranging from + 3.1 to + 13.1 points in the FACT instrument scales and + 2.3 to + 4.3 for the SF-36 subscales.
3.2.2 Novel TherapiesThe phase 2 single-arm SADAL trial (selinexor) assessed HRQOL in responders and nonresponders using the FACT-G treatment satisfaction, FACT-Lym, and FACT-Lym Trial Outcome Index (TOI) [38]. Outcomes were assessed at baseline, treatment cycles 2‒7, and the end of treatment. All patients reported decreased HRQOL at last follow-up, with responders reporting mean change scores from baseline of − 9.9 to − 6, and nonresponders reporting mean change scores of − 9.2 to − 15.7.
In the phase 3 ORCHARRD trial of ofatumumab plus dexamethasone, cytarabine, and cisplatin (DHAP) chemotherapy versus rituximab plus DHAP (R-DHAP) therapy for second-line LBCL, HRQOL was assessed using the FACT-G and FACT-Lym TOI instruments [39]. In patients treated with ofatumumab, the mean [standard error (SE)] FACT-G total score and FACT-Lym TOI decrease was − 2.561 (0.7671) and − 2.028 (0.9196), respectively. In patients treated with R-DHAP, the mean (SE) FACT-G total score and FACT-Lym TOI decrease was − 2.591 (0.7696) and − 3.156 (0.9204), respectively.
3.2.3 Salvage TherapiesOne phase 1/2, single-arm trial evaluating the clinical efficacy of rituximab plus cyclophosphamide, etoposide, and prednisone (R-CVEP) used the FACT-G and FACT-Lym instruments to measure HRQOL [40]. HRQOL improved from baseline to 12-month follow-up across all scales, with a mean change in FACT-G total score of + 11.72, FACT-Lym total score of + 18.61, and FACT-Lym TOI of + 12.29.
3.2.4 EORTC QLQ-C30 by Line of TherapyOne identified study reported HRQOL by line of therapy in a real-world setting for patients with DLBCL via a self-completed point-in-time survey using the EORTC QLQ-C30. The reported EORTC QLQ-C30 global health status score was higher for patients on second-line therapies (55.48 [18.02]) than for those on third-line and beyond therapies (49.93 [21.07]) [41].
3.3 UtilitiesSix studies were identified that assessed and reported health state utility values (Table 3).
Table 3 Overview of included studies on health statue utility values3.3.1 CAR T Cell TherapiesThree studies reported HRQOL data in patients with LBCL treated with CAR T cell therapies as follows: liso-cel (TRANSCEND NHL 001; n = 186 evaluable patients [17]), axicabtagene ciloleucel (axi-cel; ZUMA-1; n = 34 [42]), and a product-agnostic vignette-based time tradeoff study [43, 44]). In TRANSCEND NHL 001, the health utility impact of liso-cel was evaluated in eligible patients with DLBCL in the third-line or later setting using the validated EQ-5D-5L questionnaire [17, 35,36,37]. The questionnaire includes the EQ-5D-5L descriptive system and EQ-VAS. Health utilities were assessed at baseline and months 1, 2, 3, 6, 9, 12, and 18 after infusion. At baseline, the mean [standard deviation (SD)] EQ-5D-5L health state score was 0.817 (0.120). This decreased slightly at month 1 (− 0.023) and then increased from months 2 to 12 (+ 0.020 to + 0.031). At month 18, the increase from baseline in the EQ-5D-5L index score was + 0.061 (0.013). The mean (SD) score for EQ-5D-5L VAS at baseline was 68.3 (19.5), and the increase from baseline was + 10.4 (5.4) at month 18.
A phase 2 ZUMA-1 safety management study ad hoc analysis investigated the impact of axi-cel treatment on health utility patients with R/R LBCL in the third-line or later setting, as measured by the EQ-5D-5L [42]. Health utilities were assessed at screening, week 4, and months 3 and 6 after infusion. Mean (SD) EQ-5D-5L score at baseline was 0.80 (0.17). Scores at week 4 decreased slightly [0.74 (0.15); − 0.06] and then increased by month 3 [0.80 (0.13); + 0.00] and month 6 [0.82 (0.21); + 0.02]. Mean (SD) utility values by health state were 0.80 (0.14) for progression-free disease and 0.72 (0.17) for progressed disease. A disutility of 0.05 (SE, 0.04) was observed at 4 weeks, and the authors noted this was associated with the timing of CAR T cell–related adverse events (AE).
In a vignette-based time tradeoff study [43, 44], adults from the general population in the UK were surveyed to estimate the health utility impact of all-grade cytokine release syndrome (CRS) and neurological events (NE) related to CAR T cell treatment for R/R LBCL. The EQ-5D-5L was self-administered, and participants were also asked to value the following six health states: one state describing CAR T cell therapy for LBCL with no AEs, three states describing CAR T cell therapy for LBCL with varying grades of CRS, and two states describing CAR T cell therapy for LBCL with varying grades of NEs. A total of 218 participants completed the interview. The mean (SD) EQ-5D-5L index score was 0.86 (0.17) and the mean (SD) EQ-5D-5L VAS score was 82.15 (13.54) for the general population. Among the six health state vignettes valued by the general population respondents, the highest mean utility was for the health state representing CAR T cell therapy with no AEs. Disutilities per AE included grade 1 CRS (− 0.01), grade 1/2 NEs (− 0.04), grade 2 CRS (− 0.05), grade 3/4 NEs (− 0.18), and grade 3/4 CRS (− 0.23).
3.3.2 Novel TherapiesThe phase 2 single-arm SADAL trial evaluated the health utility impact of selinexor in the third-line or later setting in eligible patients with DLBCL using the validated EQ-5D-5L questionnaire [38]. Health utilities were assessed in responders and nonresponders at baseline and at cycles 2‒7. At baseline (n = 89 evaluable patients), the mean (95% CI) EQ-5D health state score was 0.789 (0.767‒0.811) for responders and 0.801 (0.781‒0.822) for nonresponders. Responders reported a mean change from baseline of − 0.010 at last follow-up, whereas nonresponders reported a mean change from baseline of − 0.274.
In the phase 1/2 CheckMate 436 trial, HRQOL was reported as an exploratory endpoint in patients with primary mediastinal B cell lymphoma treated with nivolumab combined with brentuximab vedotin in the third-line or later setting using the EQ-5D-3L [45]. HRQOL was reported at baseline, cycle 5, and for the first follow-up visit. The study reported the proportion of patients experiencing “some problems” or “extreme problems” for each dimension but did not map the results to preference-based health state utilities. The percentage of patients experiencing “some problems” with activity and pain appeared to decrease over time (− 18% and − 50%, respectively), and no clear pattern could be seen for the remaining dimensions.
The impact of naratuximab emtansine and rituximab in patients with R/R DLBCL was evaluated in a phase 2 single-arm trial using the FACT-Lym questionnaire mapped to EQ-5D index values [46]. At baseline, the mean estimated EQ-5D index score was 0.78 for responders and 0.73 for nonresponders. At the end of treatment, mean (difference) index scores were 0.77 (− 0.01) for responders and 0.67 (− 0.06) for nonresponders.
3.4 Health State Utility Values Reported in Economic Studies and HTA SubmissionsA total of 15 economic studies and seven HTA reports were identified that reported health state utility values used to inform comparative analyses of therapies for patients with R/R LBCL (Table 4). Reporting of utility values varied among HTA reports (n = 7), with six reporting values associated with progression-free and progressed states and one reporting disutility values for specified AEs (Table 5). Sources for utility values were typically clinical trials, as well as published literature. Two reports (both from the SMC) reported mapping SF-36 data to EQ-5D.
Table 4 Overview of economic studies reporting health state utility valuesTable 5 Health state utility values included in HTA reports3.4.1 CAR T Cell TherapiesEleven studies reported health state utility values used to inform cost-effectiveness models comparing CAR T cell therapies with other CAR T cell therapies (three studies) [47,48,49] or salvage chemotherapy (eight studies) [50,51,52,53,54,55,56,57] in patients with DLBCL in the third-line or later setting. These studies were conducted from a number of different perspectives, including US payer perspective [50, 51, 56, 57], Spanish National Health Service perspective [47], Singapore health care system perspective [53], Singapore private insurance payer perspective [58], Chinese health care system perspective [54], and Japanese public health care payer perspective [55]. Across these 11 studies, utility values for remission/progression-free survival ranged from 0.70 to 0.90 [50, 58], and values for disease progression ranged from 0.39 to 0.59 [47, 48, 51, 53,54,55,56,57, 59, 60]. Treatment-related utility values for CAR T cell therapies ranged from 0.50 to 0.740 [47, 48, 50, 51]. Disutilities related to treatment and AEs were reported for tisagenlecleucel: two studies [55, 57] reported treatment disutility of − 0.15 over a duration of 28 days, while disutilities related to intensive care unit stays for CRS ranged from − 0.70 to − 0.90 across three studies [53, 57, 58].
3.4.2 Novel TherapiesAmong three cost-effectiveness analyses conducted from a US payer perspective that compared polatuzumab vedotin, bendamustine, and rituximab (pola-BR) with BR (two studies) [60, 61] or tafasitamab plus lenalidomide (one study) [59], utility values were 0.83 for progression-free survival [47, 48, 50, 51, 53,54,55, 57,58,59,60,61,62] and ranged from 0.39 to 0.71 for disease progression [47, 48, 50, 51, 53,54,55, 57,58,59,60,61,62]. AE-related disutility values were − 0.02 for pola-BR and − 0.01 for tafasitamab plus lenalidomide [
留言 (0)